WHO has published guidance on adjusting public health and social measures for the next phase of the COVID-19 response.1 Some governments have suggested that the detection of antibodies to the SARS-CoV-2, the virus that causes COVID-19, could serve as the basis for an “immunity passport” or “risk-free certificate” that would enable individuals to travel or to return to work assuming that they are protected against re-infection. There is currently no evidence that people who have recovered from COVID-19 and have antibodies are protected from a second infection.
The measurement of antibodies specific to COVID-19
The development of immunity to a pathogen through natural infection is a multi-step process that typically takes place over 1-2 weeks. The body responds to a viral infection immediately with a non-specific innate response in which macrophages, neutrophils, and dendritic cells slow the progress of virus and may even prevent it from causing symptoms. This non-specific response is followed by an adaptive response where the body makes antibodies that specifically bind to the virus. These antibodies are proteins called immunoglobulins. The body also makes T-cells that recognize and eliminate other cells infected with the virus. This is called cellular immunity. This combined adaptive response may clear the virus from the body, and if the response is strong enough, may prevent progression to severe illness or re-infection by the same virus. This process is often measured by the presence of antibodies in blood.
WHO continues to review the evidence on antibody responses to SARS-CoV-2 infection.2-17 Most of these studies show that people who have recovered from infection have antibodies to the virus. However, some of these people have very low levels of neutralizing antibodies in their blood,4 suggesting that cellular immunity may also be critical for recovery. As of 24 April 2020, no study has evaluated whether the presence of antibodies to SARS-CoV-2 confers immunity to subsequent infection by this virus in humans.
Laboratory tests that detect antibodies to SARS-CoV-2 in people, including rapid immunodiagnostic tests, need further validation to determine their accuracy and reliability. Inaccurate immunodiagnostic tests may falsely categorize people in two ways. The first is that they may falsely label people who have been infected as negative, and the second is that people who have not been infected are falsely labelled as positive. Both errors have serious consequences and will affect control efforts. These tests also need to accurately distinguish between past infections from SARS-CoV-2 and those caused by the known set of six human coronaviruses. Four of these viruses cause the common cold and circulate widely. The remaining two are the viruses that cause Middle East Respiratory Syndrome and Severe Acute Respiratory Syndrome. People infected by any one of these viruses may produce antibodies that cross-react with antibodies produced in response to infection with SARS-CoV-2.
Many countries are now testing for SARS-CoV-2 antibodies at the population level or in specific groups, such as health workers, close contacts of known cases, or within households.21 WHO supports these studies, as they are critical for understanding the extent of – and risk factors associated with – infection. These studies will provide data on the percentage of people with detectable COVID-19 antibodies, but most are not designed to determine whether those people are immune to secondary infections.
Other considerations
At this point in the pandemic, there is not enough evidence about the effectiveness of antibody-mediated immunity to guarantee the accuracy of an “immunity passport” or “risk-free certificate.” People who assume that they are immune to a second infection because they have received a positive test result may ignore public health advice. The use of such certificates may therefore increase the risks of continued transmission. As new evidence becomes available, WHO will update this scientific brief.
More than $1.2 billion in federal bailout funds have been disclosed by hospitals and health systems thus far, including $150 million that was sent to Mayo Clinic, according to a review of financial documents by Axios’ Bob Herman.
Why it matters: Hospitals do not have to repay these taxpayer funds, which are supposed to offset the lost revenue and higher costs associated with handling the coronavirus outbreak. But there is no central location to track where the money is flowing.
The big picture: Hospitals and other health care providers can receive coronavirus funds through two primary sources:
Advance payments from Medicare that function as loans and must be repaid.
Where it stands: Axios has found 11 hospital organizations — ranging from small community hospitals to large, multistate systems — that have disclosed bailout funding and Medicare loans through municipal bondholder documents or public filings, and compiled them into a database.
Some of the largest bailout payments disclosed so far have gone to HCA Healthcare ($700 million), Mayo Clinic ($150 million), Mercy ($101.7 million) and NYU Langone Health ($73.1 million).
$50 billion of the first $100 billion in bailout funds is “allocated proportional to providers’ share of 2018 net patient revenue,” according to HHS, and therefore likely favors systems that are bigger and/or charge higher prices.
Medicare has sent $100 billion as loans as of April 24, $7 billion of which has been disclosed to these 11 hospital systems.
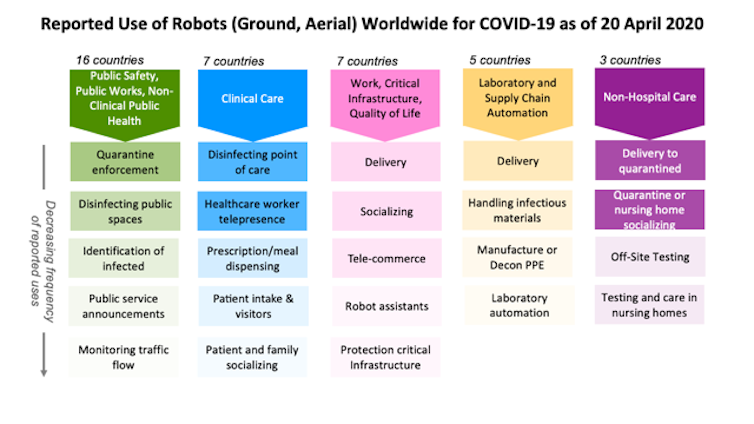
These are just a few of the two dozen ways robots have been used during the COVID-19 pandemic, from health care in and out of hospitals, automation of testing, supporting public safety and public works, to continuing daily work and life.
The lessons they’re teaching for the future are the same lessons learned at previous disasters but quickly forgotten as interest and funding faded. The best robots for a disaster are the robots, like those in these examples, that already exist in the health care and public safety sectors.
Research laboratories and startups are creating new robots, including one designed to allow health care workers to remotely take blood samples and perform mouth swabs. These prototypes are unlikely to make a difference now. However, the robots under development could make a difference in future disasters if momentum for robotics research continues.
Robots around the world
As roboticists at Texas A&M University and the Center for Robot-Assisted Search and Rescue, we examined over 120 press and social media reports from China, the U.S. and 19 other countries about how robots are being used during the COVID-19 pandemic. We found that ground and aerial robots are playing a notable role in almost every aspect of managing the crisis.
At work and home, robots are assisting in surprising ways. Realtors are teleoperating robots to show properties from the safety of their own homes. Workers building a new hospital in China were able work through the night because drones carried lighting. In Japan, students used robots to walk the stage for graduation, and in Cyprus, a person used a drone to walk his dog without violating stay-at-home restrictions.
Helping workers, not replacing them
Every disaster is different, but the experience of using robots for the COVID-19 pandemic presents an opportunity to finally learn three lessons documented over the past 20 years. One important lesson is that during a disaster robots do not replace people. They either perform tasks that a person could not do or do safely, or take on tasks that free up responders to handle the increased workload.
The majority of robots being used in hospitals treating COVID-19 patients have not replaced health care professionals. These robots are teleoperated, enabling the health care workers to apply their expertise and compassion to sick and isolated patients remotely.
A small number of robots are autonomous, such as the popular UVD decontamination robots and meal and prescription carts. But the reports indicate that the robots are not displacing workers. Instead, the robots are helping the existing hospital staff cope with the surge in infectious patients. The decontamination robots disinfect better and faster than human cleaners, while the carts reduce the amount of time and personal protective equipment nurses and aides must spend on ancillary tasks.
Off-the-shelf over prototypes
The second lesson is the robots used during an emergency are usually already in common use before the disaster. Technologists often rush out well-intentioned prototypes, but during an emergency, responders – health care workers and search-and-rescue teams – are too busy and stressed to learn to use something new and unfamiliar. They typically can’t absorb the unanticipated tasks and procedures, like having to frequently reboot or change batteries, that usually accompany new technology.
Fortunately, responders adopt technologies that their peers have used extensively and shown to work. For example, decontamination robots were already in daily use at many locations for preventing hospital-acquired infections. Sometimes responders also adapt existing robots. For example, agricultural drones designed for spraying pesticides in open fields are being adapted for spraying disinfectants in crowded urban cityscapes in China and India.
Workers in Kunming City, Yunnan Province, China refill a drone with disinfectant. The city is using drones to spray disinfectant in some public areas.Xinhua News Agency/Yang Zongyou via Getty Images
A third lesson follows from the second. Repurposing existing robots is generally more effective than building specialized prototypes. Building a new, specialized robot for a task takes years. Imagine trying to build a new kind of automobile from scratch. Even if such a car could be quickly designed and manufactured, only a few cars would be produced at first and they would likely lack the reliability, ease of use and safety that comes from months or years of feedback from continuous use.
Alternatively, a faster and more scalable approach is to modify existing cars or trucks. This is how robots are being configured for COVID-19 applications. For example, responders began using the thermal cameras already on bomb squad robots and drones – common in most large cities – to detect infected citizens running a high fever. While the jury is still out on whether thermal imaging is effective, the point is that existing public safety robots were rapidly repurposed for public health.
Don’t stockpile robots
The broad use of robots for COVID-19 is a strong indication that the health care system needed more robots, just like it needed more of everyday items such as personal protective equipment and ventilators. But while storing caches of hospital supplies makes sense, storing a cache of specialized robots for use in a future emergency does not.
This was the strategy of the nuclear power industry, and it failed during the Fukushima Daiichi nuclear accident. The robots stored by the Japanese Atomic Energy Agency for an emergency were outdated, and the operators were rusty or no longer employed. Instead, the Tokyo Electric Power Company lost valuable time acquiring and deploying commercial off-the-shelf bomb squad robots, which were in routine use throughout the world. While the commercial robots were not perfect for dealing with a radiological emergency, they were good enough and cheap enough for dozens of robots to be used throughout the facility.
Robots in future pandemics
Hopefully, COVID-19 will accelerate the adoption of existing robots and their adaptation to new niches, but it might also lead to new robots. Laboratory and supply chain automation is emerging as an overlooked opportunity. Automating the slow COVID-19 test processing that relies on a small set of labs and specially trained workers would eliminate some of the delays currently being experienced in many parts of the U.S.
Automation is not particularly exciting, but just like the unglamorous disinfecting robots in use now, it is a valuable application. If government and industry have finally learned the lessons from previous disasters, more mundane robots will be ready to work side by side with the health care workers on the front lines when the next pandemic arrives.
“CAME OUT of nowhere,” President Trump said March 6 of the coronavirus pandemic. “I just think this is something . . . that you can never really think is going to happen.” A few weeks later, he added, “I would view it as something that just surprised the whole world.” Mr. Trump also said, “Nobody knew there would be a pandemic or epidemic of this proportion.”
Of course, no one can pinpoint the exact moment that lightning will strike. But a global pandemic? Experts have predicted it, warned about the preparedness gaps and urged action. Again and again and again.
Just look at 2019. In January, the U.S. intelligence community issued its annual global threat assessment. It declared, “We assess that the United States and the world will remain vulnerable to the next flu pandemic or large-scale outbreak of a contagious disease that could lead to massive rates of death and disability, severely affect the world economy, strain international resources, and increase calls on the United States for support. . . . The growing proximity of humans and animals has increased the risk of disease transmission. The number of outbreaks has increased in part because pathogens originally found in animals have spread to human populations.”
In September, the Johns Hopkins Center for Health Security issued a report titled “Preparedness for a High-Impact Respiratory Pathogen Pandemic.” The report found that if such a pathogen emerged, “it would likely have significant public health, economic, social, and political consequences. . . . The combined possibilities of short incubation periods and asymptomatic spread can result in very small windows for interrupting transmission, making such an outbreak difficult to contain.” The report pointed to “large national and international readiness gaps.”
In October, the Nuclear Threat Initiative, working with the Johns Hopkins center and the Economist Intelligence Unit, published its latest Global Health Security Index, examining open-source information about the state of health security across 195 nations, and scoring them. The report warned, “No country is fully prepared for epidemics or pandemics, and every country has important gaps to address.” The report found that “Fewer than 5 percent of countries scored in the highest tier for their ability to rapidly respond to and mitigate the spread of an epidemic.”
In November, the Center for Strategic and International Studies published a study by its Commission on Strengthening America’s Health Security. It warned, “The American people are far from safe. To the contrary, the United States remains woefully ill-prepared to respond to global health security threats. This kind of vulnerability should not be acceptable to anyone. At the extreme, it is a matter of life and death. . . . Outbreaks proliferate that can spread swiftly across the globe and become pandemics, disrupting supply chains, trade, transport, and ultimately entire societies and economies.” The report recommended: “Restore health security leadership at the White House National Security Council.”
Came out of nowhere? Not even close. The question that must be addressed in future postmortems is why all this expertise and warning was ignored.
The pandemic is a long way from over, and its impact on our daily lives, information ecosystem, politics, cities and health care will last even longer.
The big picture: The novel coronavirus has infected more than 939,000 people and killed over 54,000 in the U.S., Johns Hopkins data shows. More than 105,000 Americans have recovered from the virus as of Sunday.
Lockdown measures: Demonstrators gathered in Florida, Texas and Louisiana Saturday to protest stay-at-home orders designed to protect against the spread of COVID-19, following a week of similar rallies across the U.S.
16 states have released formal reopening plans, Vice President Mike Pence said at Thursday’s White House briefing. Several Southern states including South Carolina have already begun reopening their economies.
Alaska, Oklahoma and Georgiareopened some non-essential businesses Friday. President Trump said Wednesday he “strongly” disagrees with Georgia Gov. Brian Kemp on the move.
California’s stay-at-home orders and business restrictions will remain in place,Gov. Gavin Newsom made clear at a Wednesday news briefing. But some local authorities reopened beaches in Southern California Saturday.
New York recorded its third-straight day of fewer coronavirus deaths Friday. Still, Gov. Andrew Cuomo said he’s not willing to reopen the state, citing CDC guidance that states need two weeks of flat or declining numbers.
Catch up quick: Deborah Birx said Sunday that it “bothers” her that the news cycle is still focused on Trump’s comments about disinfectants possibly treating coronavirus, arguing that “we’re missing the bigger pieces” about how Americans can defeat the virus.
Anthony Fauci said Saturday the U.S. is testing roughly 1.5 million to 2 million people a week. “We probably should get up to twice that as we get into the next several weeks, and I think we will,” he said.
The number of sailors aboard the USS Kidd to test positive for the coronavirus has risen from 18 Friday to 33, the U.S. Navy said Saturday. It’s the second major COVID-19 outbreak on a U.S. naval vessel, after the USS Theodore Roosevelt, where a total of 833 crew members tested positive, per the Navy’s latest statement.
The first personknown to have the coronavirus when they died was killed by a heart attack “due to COVID-19 infection” on Feb. 6, autopsy results obtained by the San Francisco Chronicle on Saturday show.
By the numbers: The coronavirus has infected over 2.9 million people and killed over 200,000, Johns Hopkins data shows. More than 829,000 people have recovered from COVID-19. The U.S. has reported the most cases in the world (more than 940,000 from 5.1 million tests), followed by Spain (over 223,000).
What’s happening: Australian Health Minister Greg Hunt announced a new coronavirus tracing app on Sunday that the government hopes at least 50 percent of the population will use. A top health official said the app is “only for one purpose, to help contact tracing,” as he sought to reassure Australians on privacy issues.
Argentina is extending a nationwide shelter-in-place order that was due to expire Sunday until May 10, President Alberto Fernandez said on Saturday, per Reuters. The country has confirmed over 3,700 cases, according to Johns Hopkins.
Spain will gradually ease nationwide stay-at-home restrictions starting May 2 if coronavirus cases continue to decline, Prime Minister Pedro Sánchez said Saturday.
The World Health Organization said Saturday there is “no evidence” that people who recover from COVID-19 and have antibodies are protected from a second infection.
India announced it will be easing lockdown measures for its 1.3 billion people in the areas outside of hotspots — providing some relief for locally owned businesses and daily wage workers.
The director of Israel’s foreign intelligence agency, Mossad, said in a briefing to health care officials on Thursday that Iran and its regional allies are intentionally underreporting cases and deaths from the coronavirus.
New Zealand’s level 4 lockdown measures requiring non-essential workers to stay home have been extended to 11:59 p.m next Monday, when the country moves into a still-strict level 3. NZ reported just three cases on Thursday.
Pakistan has decided to keep mosques open during the fasting month of Ramadan, which began Thursday, as cases continue to climb, AP reports.
The big picture: The world faces its gravest challenge in decades, but geopolitical tensions won’t wait until it’s over. Trump’s threat on Wednesday to “destroy” Iranian boats that harass U.S. ships comes amid arrests of Hong Kong pro-democracy activists and clashes in Afghanistan that could further undermine peace there.
By the numbers: The coronavirus has infected over 2.9 million people and killed over 200,000, Johns Hopkins data shows. More than 829,000 people have recovered from COVID-19. The U.S. has reported the most cases in the world (more than 940,000 from 5.1 million tests), followed by Spain (over 223,000).
The coronavirus pandemic is shaking bedrock assumptions about U.S. exceptionalism. This is perhaps the first global crisis in more than a century where no one is even looking for Washington to lead.
As images of America’s overwhelmed hospital wards and snaking jobless lines have flickered across the world, people on the European side of the Atlantic are looking at the richest and most powerful nation in the world with disbelief.
“When people see these pictures of New York City they say, ‘How can this happen? How is this possible?’” said Henrik Enderlein, president of the Berlin-based Hertie School, a university focused on public policy. “We are all stunned. Look at the jobless lines. Twenty-two million,” he added.
“I feel a desperate sadness,” said Timothy Garton Ash, a professor of European history at Oxford University and a lifelong and ardent Atlanticist.
The pandemic sweeping the globe has done more than take lives and livelihoods from New Delhi to New York. It is shaking fundamental assumptions about American exceptionalism — the special role the United States played for decades after World War II as the reach of its values and power made it a global leader and example to the world.
Today it is leading in a different way: More than 840,000 Americans have been diagnosed with Covid-19 and at least 46,784 have died from it, more than anywhere else in the world.
As the calamity unfolds, President Trump and state governors are not only arguing over what to do, but also over who has the authority to do it. Mr. Trump has fomented protests against the safety measures urged by scientific advisers, misrepresented facts about the virus and the government response nearly daily, and this week used the virus to cut off the issuing of green cards to people seeking to emigrate to the United States.
“America has not done badly, it has done exceptionally badly,” said Dominique Moïsi, a political scientist and senior adviser at the Paris-based Institut Montaigne.
And in the United States, it has exposed two great weaknesses that, in the eyes of many Europeans, have compounded one another: the erratic leadership of Mr. Trump, who has devalued expertise and often refused to follow the advice of his scientific advisers, and the absence of a robust public health care system and social safety net.
“America prepared for the wrong kind of war,” Mr. Moïsi said. “It prepared for a new 9/11, but instead a virus came.”
“It raises the question: Has America become the wrong kind of power with the wrong kind of priorities?” he asked.
Ever since Mr. Trump moved into the White House and turned America First into his administration’s guiding mantra, Europeans have had to get used to the president’s casual willingness to risk decades-old alliances and rip up international agreements. Early on, he called NATO “obsolete” and withdrew U.S. support from the Paris climate agreement and the Iran nuclear deal.
But this is perhaps the first global crisis in more than a century where no one is even looking to the United States for leadership.
In Berlin, Germany’s foreign minister, Heiko Maas, has said as much.
China took “very authoritarian measures, while in the U.S., the virus was played down for a long time,” Mr. Maas recently told Der Spiegel magazine.
“These are two extremes, neither of which can be a model for Europe,” Mr. Maas said.
America once told a story of hope, and not just to Americans. West Germans like Mr. Maas, who grew up on the front line of the Cold War, knew that story by heart, and like many others in the world, believed it.
But nearly three decades later, America’s story is in trouble.
The country that helped defeat fascism in Europe 75 years ago next month, and defended democracy on the continent in the decades that followed, is doing a worse job of protecting its own citizens than many autocracies and democracies.
There is a special irony: Germany and South Korea, both products of enlightened postwar American leadership, have become potent examples of best practices in the coronavirus crisis.
But critics now see America failing not only to lead the world’s response, but letting down its own people as well.
“There is not only no global leadership, there is no national and no federal leadership in the United States,” said Ricardo Hausmann, director of the Growth Lab at Harvard’s Center for International Development. “In some sense this is the failure of leadership of the U.S. in the U.S.”
Of course, some countries in Europe have also been overwhelmed by the virus, with the number of dead from Covid-19 much higher as a percentage of the population in Italy, Spain and France than in the United States. But they were struck sooner and had less time to prepare and react.
The contrast between how the United States and Germany responded to the virus is particularly striking.
While Chancellor Angela Merkel has been criticized for not taking a forceful enough leadership role in Europe, Germany is being praised for a near-textbook response to the pandemic, at least by Western standards. That is thanks to a robust public health care system, but also a strategy of mass testing and trusted and effective political leadership.
Ms. Merkel has done what Mr. Trump has not. She has been clear and honest about the risks with voters and swift in her response. She has rallied all 16 state governors behind her. A trained physicist, she has followed scientific advice and learned from best practice elsewhere.
Not long ago, Ms. Merkel was considered a spent force, having announced that this would be her last term. Now her approval ratings are at 80 percent.
“She has the mind of a scientist and the heart of a pastor’s daughter,” Mr. Garton Ash said.
Mr. Trump, in a hurry to restart the economy in an election year, has appointed a panel of business executives to chart a course out of the lockdown.
Ms. Merkel, like everyone, would like to find a way out, too, but this week she warned Germans to remain cautious. She is listening to the advice of a multidisciplinary panel of 26 academics from Germany’s national academy of science. The panel includes not just medical experts and economists but also behavioral psychologists, education experts, sociologists, philosophers and constitutional experts.
“You need a holistic approach to this crisis,” said Gerald Haug, the academy’s president, who chairs the German panel. “Our politicians get that.”
A climatologist, Mr. Haug used to do research at Columbia University in New York.
The United States has some of the world’s best and brightest minds in science, he said. “The difference is, they’re not being listened to.”
“It’s a tragedy,” he added.
Some cautioned that the final history of how countries fare after the pandemic is still a long way from being written.
A pandemic is a very specific kind of stress test for political systems, said Mr. Garton Ash, the history professor. The military balance of power has not shifted at all. The United States remains the world’s largest economy. And it was entirely unclear what global region would be best equipped to kick-start growth after a deep recession.
“All of our economies are going to face a terrible test,” he said. “No one knows who will come out stronger at the end.”
Benjamin Haddad, a French researcher at the Atlantic Council, wrote that while the pandemic was testing U.S. leadership, it is “too soon to tell” if it would do long-term damage.
“It is possible that the United States will resort to unexpected resources, and at the same time find a form of national unity in its foreign policy regarding the strategic rivalry with China, which it has been lacking until now,” Mr. Haddad wrote.
There is another wild card in the short term, Mr. Moïsi pointed out. The United States has an election in November. That, and the aftermath of the deepest economic crisis since the 1930s, might also affect the course of history.
The Great Depression gave rise to America’s New Deal. Maybe the coronavirus will lead the United States to embrace a stronger public safety net and develop a national consensus for more accessible health care, Mr. Moïsi suggested.
“Europe’s social democratic systems are not only more human, they leave us better prepared and fit to deal with a crisis like this than the more brutal capitalistic system in the United States,” Mr. Moïsi said.
The current crisis, some fear, could act like an accelerator of history, speeding up a decline in influence of both the United States and Europe.
“Sometime in 2021 we come out of this crisis and we will be in 2030,” said Mr. Moïsi. “There will be more Asia in the world and less West.”
Mr. Garton Ash said that the United States should take an urgent warning from a long line of empires that rose and fell.
“To a historian it’s nothing new, that’s what happens,” said Mr. Garton Ash. “It’s a very familiar story in world history that after a certain amount of time a power declines.”
“You accumulate problems, and because you’re such a strong player, you can carry these dysfunctionalities for a long time,” he said. “Until something happens and you can’t anymore.”
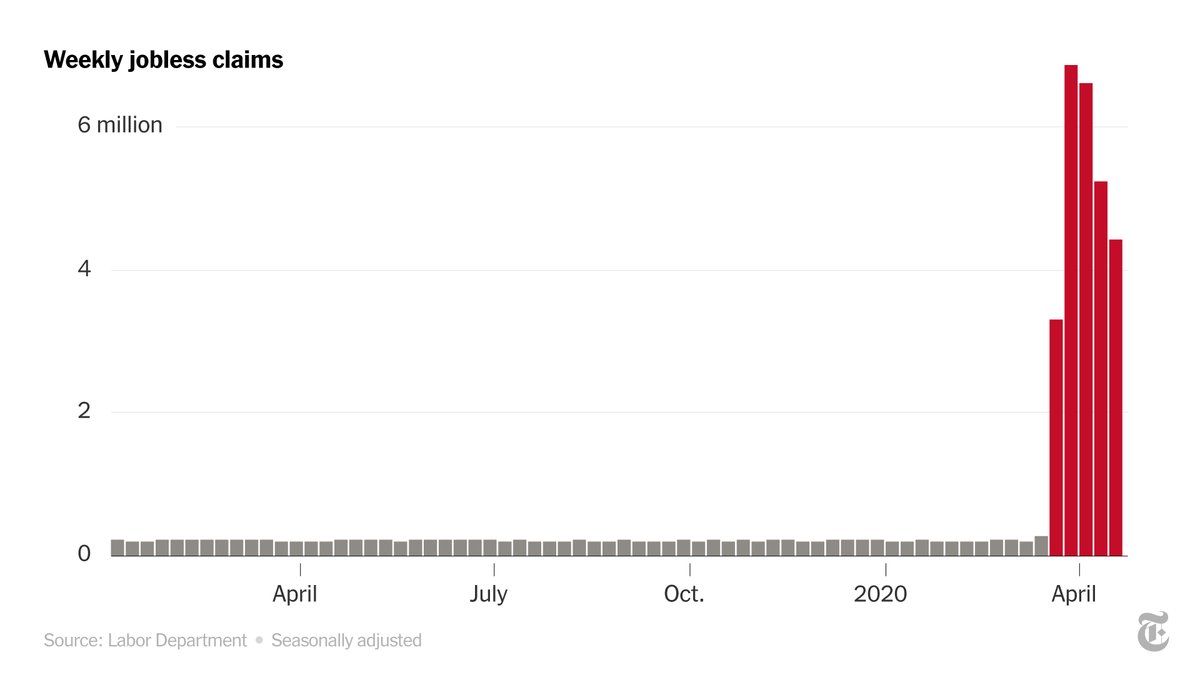
With 4.4 million added last week, the five-week total passed 26 million. The struggle by states to field claims has hampered economic recovery.
Nearly a month after Washington rushed through an emergency package to aid jobless Americans, millions of laid-off workers have still not been able to apply for those benefits — let alone receive them — because of overwhelmed state unemployment systems.
Across the country, states have frantically scrambled to handle a flood of applications and apply a new set of federal rules even as more and more people line up for help. On Thursday, the Labor Department reported that another 4.4 million people filed initial unemployment claims last week, bringing the five-week total to more than 26 million.
“At all levels, it’s eye-watering numbers,” Torsten Slok, chief international economist at Deutsche Bank Securities, said. Nearly one in six American workers has lost a job in recent weeks.
Delays in delivering benefits, though, are as troubling as the sheer magnitude of the figures, he said. Such problems not only create immediate hardships, but also affect the shape of the recovery when the pandemic eases.
Laid-off workers need money quickly so that they can continue to pay rent and credit card bills and buy groceries. If they can’t, Mr. Slok said, the hole that the larger economy has fallen into “gets deeper and deeper, and more difficult to crawl out of.”
Hours after the Labor Department report, the House passed a $484 billion coronavirus relief package to replenish a depleted small-business loan program and fund hospitals and testing. The Senate approved the bill earlier this week.
Even as Congress continues to provide aid, distribution has remained challenging. According to the Labor Department, only 10 states have started making payments under the federal Pandemic Unemployment Assistance program, which extends coverage to freelancers, self-employed workers and part-timers. Most states have not even completed the system needed to start the process.
Ohio, for example, will not start processing claims under the expanded federal eligibility criteria until May 15. Recipients whose state benefits ran out, but who can apply for extended federal benefits, will not begin to have their claims processed until May 1.
Pennsylvania opened its website for residents to file for the federal program a few days ago, but some applicants were mistakenly told that they were ineligible after filling out the forms. The state has given no timetable for when benefits might be paid.
Reports of delays, interruptions and glitches continue to come in from workers who have been unable to get into the system, from others who filed for regular state benefits but have yet to receive them, and from applicants who say they have been unfairly turned down and unable to appeal.
“Speed matters” when it comes to government assistance, said Carl Tannenbaum, chief economist at Northern Trust. Speed can mean the difference between a company’s survival and its failure, or between making a home mortgage payment and facing foreclosure.
There is “a race between policy and a pandemic,” Mr. Tannenbaum said, and in many places, it is clear that the response has been “very uneven.”
Using data reported by the Labor Department for March 14 to April 11, the Economic Policy Institute, a liberal research group, estimated that seven in 10 applicants were receiving benefits. That left seven million other jobless workers who had filed claims but were still waiting for relief.
States manage their own unemployment insurance programs and set the level of benefits and eligibility rules. Now they are responsible for administering federal emergency benefits that provide payments for an additional 13 weeks, cover previously ineligible workers and add $600 to the regular weekly check.
So far, 44 states have begun to send the $600 supplement to jobless workers who qualified under state rules, the Labor Department said. Only two — Kentucky and Minnesota — have extended federal benefits to workers who have used up their state allotment.
With government phones and websites clogged and drop-in centers closed, legal aid lawyers around the country are fielding complaints from people who say they don’t know where else to turn.
“Our office has received thousands of calls,” said John Tirpak, a lawyer with the Unemployment Law Project, a nonprofit group in Washington.
People with disabilities and nonnative English speakers have had particular problems, he said.
Even those able to file initially say they have had trouble getting back into the system as required weekly to recertify their claims.
Colin Harris of Marysville, Wash., got a letter on March 31 from the state’s unemployment insurance office saying he was eligible for benefits after being laid off as a quality inspector at Safran Cabin, an aerospace company. He submitted claims two weeks in a row and heard nothing. When he submitted his next claim, he was told that he had been disqualified. He has tried calling more than 200 times since then, with no luck.
“And that’s still where I am right now,” he said, “unable to talk to somebody to find out what the issue is.” If he had not received a $1,200 stimulus check from the federal government, he said, he would not have been able to make his mortgage payment.
Last week’s tally of new claims was lower than each of the previous three weeks. But millions of additional claims are still expected to stream in from around the country over the next month, while hiring remains piddling.
States are frantically trying to catch up. California, which has processed 2.7 million claims over the last four weeks, opened a second call center on Monday. New York, which has deployed 3,100 people to answer the telephone, said this week that it had reduced the backlog that accumulated by April 8 to 4,305 from 275,000.
Florida had the largest increase in initial claims last week, although the state figures, unlike the national total, are not seasonally adjusted. That increase could be a sign that jobless workers finally got access to the system after delays, but it is impossible to assess how many potential applicants have still failed to get in.
The 10 states that have started making Pandemic Unemployment Assistance payments to workers who would not normally qualify under state guidelines are Alabama, Colorado, Iowa, Kentucky, Louisiana, Massachusetts, Rhode Island, Tennessee, Texas and Utah.
Pain is everywhere, but it is most widespread among the most vulnerable.
In a survey that the Pew Research Center released on Tuesday, 52 percent of low-income households — below $37,500 a year for a family of three — said someone in the household had lost a job because of the coronavirus, compared with 32 percent of upper-income ones (with earnings over $112,600). Forty-two percent of families in the middle have been affected as well.
Those without a college education have taken a disproportionate hit, as have Hispanics and African-Americans, the survey found.
An outsize share of jobless claims have also been filed by women, according to an analysis from the Fuller Project, a nonprofit journalism organization that focuses on women.
Josalyn Taylor, 31, learned that she was out of a job on March 16. “I clocked in at 3 o’clock, and by 3:30 my boss called me and told me we were going to shut down for three weeks,” said Ms. Taylor, an assistant manager at Cicis Pizza in Galveston, Tex. The restaurant has yet to reopen.
Two days later, she applied for unemployment insurance, but she kept receiving a message that a claim was already active for her Social Security number and that she could not file. She has tried to clear up the matter hundreds of times — online, by phone and through the Texas Workforce Commission’s site on Facebook — with no luck.
“I used my stimulus check to pay my light bill, and I’m using that to keep groceries and stuff in the house,” said Ms. Taylor, who is five months pregnant. “But other than that, I don’t have any other income, and I’m almost out of money.”
The first wave of layoffs most heavily whacked the restaurant, travel, personal care, retail and manufacturing industries, but the damage has spread to a much broader range of sectors.
At the online job site Indeed, for example, postings for software development jobs are down nearly 30 percent from last year, while listings for finance and banking openings are down more than 40 percent.
New layoffs are expected to ease over the next couple of months, but the damage to the economy is likely to last much longer. In a matter of weeks, the shutdown has more than erased 10 years of net job gains — more than 19 million jobs.
Health and education are going to revive relatively quickly, said Rick Rieder, chief investment officer for global fixed income at BlackRock, but leisure and hospitality are going to take a lot longer.
“A lot of the people who have been furloughed won’t come back,” he said. “Companies will either close or decide not to take back those workers.”
Over the past decade, the employment landscape has shifted substantially as new types of jobs have appeared and old categories have disappeared. The U.S. economy, Mr. Rieder said, is “going to go through another period of evolution.”
National physician staffing firm Envision Healthcare is considering filing for bankruptcy, according a report from Bloomberg. Sources say the company, backed by private equity (PE) firm KKR, which acquired Envision for $9.9B in June 2018, has hired restructuring advisors and is working with an investment bank. The abrupt halt to elective surgeries and reduction in emergency room volumes due to COVID-19 has caused Envision’s business to shrink by 65 to 75 percent in just two weeks at its 168 open ambulatory surgery centers (ASCs), compared to the same time period last year.
The Nashville-based company, which employs over 25,000 physicians and advanced practitioners, has already been reducing pay for providers and executives, in addition to implementing temporary furloughs. Envision is also struggling with a debt load of more than $7B, resulting from its 2018 leveraged buyout, and has been unable to convince its bondholders to approve a debt swap.
It remains to be seen whether Envision will be a bellwether for how other PE-backed physician groups will weather the ongoing COVID crisis. While Envision’s composition of mainly hospital- and ASC-based providers, coupled with its huge debt load, leave it on especially shaky financial footing, many PE-backed physician groups will struggle this year to achieve anything close to the 20 percent annual rate of return often promised to investors.
If high-profile PE-backed groups like Envision end up declaring bankruptcy, it will likely impact the calculus of the many independent practices which may have previously looked to PE firms for acquisition, andtemper the enthusiasm of investors, who might see physician staffing and practice roll-ups as less attractive as volumes continue to fluctuate.