
Relatively few Americans say they have been diagnosed with COVID-19 or tested positive for coronavirus antibodies, but many more believe they may have been infected or say they personally know someone who has been diagnosed.
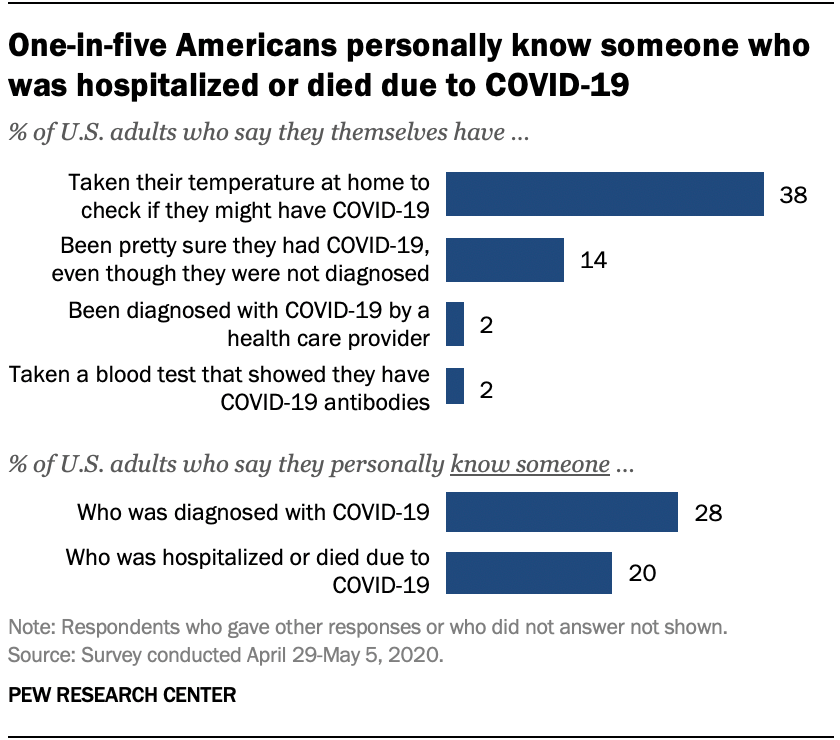
Only 2% of U.S. adults say they have been officially diagnosed with COVID-19 by a health care provider, according to a new Pew Research Center survey. And 2% say they have taken a blood test that showed they have COVID-19 antibodies, an indication that they previously had the coronavirus. But many more Americans (14%) say they are “pretty sure” they had COVID-19, despite not getting an official diagnosis. And nearly four-in-ten (38%) say they’ve taken their temperature to check if they might have the disease.
Although few Americans have been diagnosed with COVID-19 themselves, many more say they know someone with a positive diagnosis. More than one-in-four U.S. adults (28%) say they personally know someone who has been diagnosed by a health care provider as having COVID-19. A smaller share of Americans (20%) say they know someone who has been hospitalized or who has died as a result of having the coronavirus.
Some groups are more likely than others to report personal experiences with COVID-19. For instance, black adults are the most likely to personally know someone who has been hospitalized or died as a result of the disease. One-third of black Americans (34%) know someone who has been hospitalized or died, compared with 19% of Hispanics and 18% of white adults. Black Americans (32%) are also slightly more likely than Hispanic adults (26%) to know someone diagnosed with COVID-19. Public health studies have found black Americans are disproportionately dying or requiring hospitalization as a result of the coronavirus.

Areas in the northeastern United States have recorded some of the highest rates of coronavirus cases and fatalities, and this is reflected in the Center’s survey. About four-in-ten adults living in the Northeast (42%) say they personally know someone diagnosed with COVID-19, significantly more than among adults living in any other region. People living in the Northeast (31%) are also the most likely to know someone who has been hospitalized or died as a result of the disease.
One aspect of personal risk for exposure to the coronavirus is whether someone is employed in a setting where they must have frequent contact with other people, such as at a grocery store, hospital or construction site. Given the potential for the spread of the coronavirus within households, risk to individuals is also higher if other members of the household are employed in similar settings. Among people who are currently employed full-time, 35% are working in a job with frequent public contact. Among those working part-time, almost half work (48%) in such a setting. For those living in a household with other adults, 35% report that at least one of those individuals is working in a job that requires frequent contact with other people.
Taken together, nearly four-in-ten Americans (38%) have this type of exposure – either currently working in a job that requires contact with others, living in a household with others whose jobs require contact, or both.
Hispanics (at 48%) are more likely than either blacks (38%) or whites (35%) to have this type of personal or household exposure. An earlier Center analysis of government data found Hispanic adults were slightly more likely to work in service-sector jobs that require customer interaction, and that are at higher risk of layoffs as a result of the virus. In fact, the current Center survey found Hispanics were among the most likely to have experienced pay cuts or job losses due to the coronavirus outbreak.

Interpersonal exposure in the workplace is also more widespread among younger adults. And there is a 10 percentage point difference between upper- and lower-income Americans in exposure, with lower-income adults more likely to work in situations where they have to interact with the public, or to live with people who do.
Health experts warn that COVID-19 is particularly dangerous to people who have underlying medical conditions. In the survey, one-third of adults say they have such a condition. Among this group, nearly six-in-ten (58%) say that the coronavirus outbreak is a major threat to their personal health. Among those who do not report having an underlying medical condition, just 28% see the outbreak as a major threat to their health. Americans who have an underlying health condition are also more likely than those who do not to say they’ve taken their temperature to check if they might have COVID-19 (47% vs. 33% of those without a health condition).
Self-reports of an underlying health condition vary greatly by age. Among those ages 18 to 29, just 16% say they have a condition; this rises steadily with age to 56% among those 65 and older. Whites are a little more likely than blacks and Hispanics to report having a health condition, but both blacks (at 54%) and Hispanics (52%) are far more likely than whites (32%) to say that the coronavirus outbreak is “a major threat” to their health.









