
https://www.ranker.com/list/maps-mash-v1/mel-judson?format=slideshow&slide=1
Category Archives: Pandemic
Coronavirus cases could reach 150,000 a day this fall, widely followed Morgan Stanley analyst says

KEY POINTS
- Morgan Stanley’s biotechnology analyst, Matthew Harrison, said 150,000 daily new U.S. coronavirus cases are possible in the fall without better control of the virus.
- The analyst has gained a wide following on Wall Street for his success in predicting the course of the pandemic and government responses.
- Harrison previously projected a “second wave” in the fall with daily new cases between 40,000 and 50,000 nationwide.
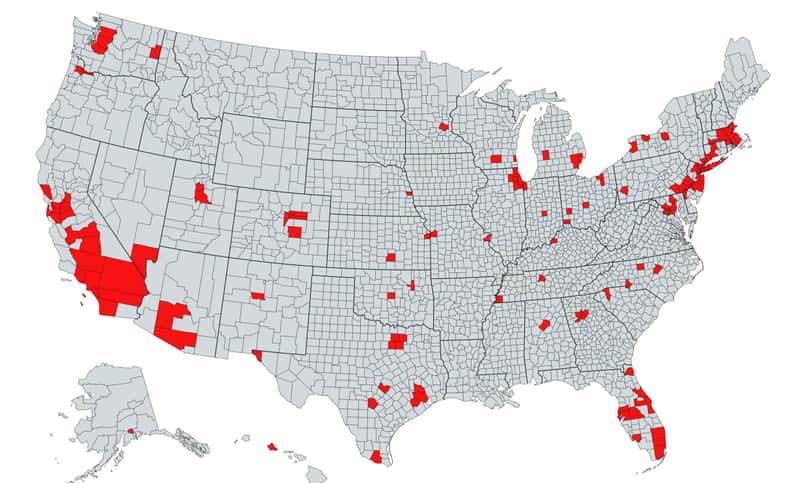
- However, the recent hot spots — Arizona, Texas, Florida and California — have shown a high rate of infection, which led the analyst to adjust to a more pessimistic view on the pandemic.

The spread of the coronavirus could be elevated this fall with as many as 150,000 daily cases in the U.S., according to Morgan Stanley’s biotechnology analyst, Matthew Harrison.
“We update our scenarios to account for the higher sustained infection rate,” Harrison said in a note Thursday. “Our bull [most optimistic] case reflects similar virus control to Europe while our base [most likely] case assumes a near-term plateau followed by increased spread in the fall. [About] 150,000 daily new cases are possible without better control of the virus.”
Harrison previously projected a “second wave” in the autumn with daily new cases totaling between 40,000 and 50,000 nationwide. However, the recent emergence of hot spots — Arizona, Texas, Florida and California — has reflected a high rate of infection, which led the analyst to adjust to a more pessimistic view on the pandemic.
The analyst has gained a wide following on Wall Street for his success in predicting the course of the pandemic and government responses. For example, in April, Harrison warned that the reopening of the U.S. economy would be a slow and tedious process.
“Our assumption of a growing reproduction number, and consequently increasing daily cases, throughout the rest of the year is based on the fact that traditionally the spread of viruses is elevated in the fall compared to the summer primarily due to more people in enclosed spaces,” Harrison said.
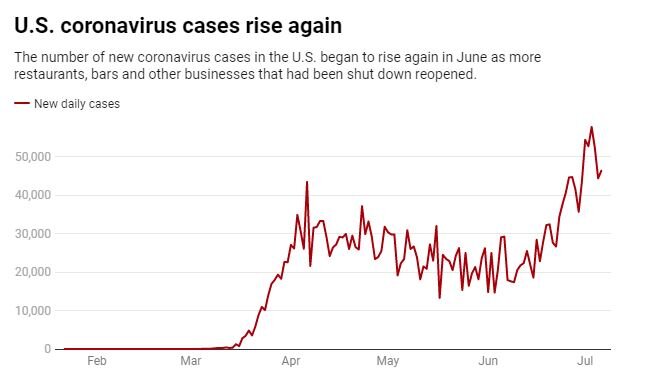
A recent resurgence in new cases has forced a number of states to roll back their reopening plans, which weighed on the stock market that rallied massively in the second quarter on hopes for a fast economic recovery.
Texas and Florida hit grim records earlier this week for daily coronavirus deaths based on a seven-day moving average.The virus has infected an average of 66,805 people per day in the U.S. over the past seven days, up more than 7% compared with a week ago, according to a CNBC analysis of data compiled by Johns Hopkins University.
On Wednesday, California reported a record spike in daily infections and passed New York as the U.S. state with the most confirmed infections since the pandemic began.
To be sure, Harrison said his projection doesn’t take into account any pharmacological intervention such as vaccines or strict lockdown measures that could potentially dampen the infection rate.
There has been a slew of positive news on the vaccine front this week. The U.S. agreed to pay drugmaker Pfizer and German partner BioNTech nearly $2 billion for 100 million coronavirus vaccines if their candidate proves both safe and effective.
Meanwhile, another vaccine candidate from Oxford University and AstraZeneca showed a positive immune response in an early trial. Earlier this week, British pharmaceutical company Synairgen claimed that its new respiratory coronavirus treatment has reduced the number of hospitalized Covid-19 patients needing intensive care in a clinical trial.
Goldman Sachs biotech analyst Salveen Richter said the Covid-19 vaccine market will be similar to the flu vaccine market, which requires an annual or periodic vaccination. The analyst also cited data showing the global vaccine market will grow to at least $40 billion in 2023 from $35 billion in 2018.
Fauci on coronavirus: ‘I don’t really see us eradicating it’
Anthony Fauci, the nation’s top infectious diseases expert, said Wednesday he doesn’t think COVID-19 will ever be fully eradicated but noted it can be controlled.
“I don’t see this disappearing the way SARS 1 did,” Fauci said during a livestreamed event hosted by the TB Alliance, a nonprofit focused on finding better tuberculosis treatments.
The SARS outbreak that started in 2003 lasted several months and mostly affected Asian countries before eventually vanishing. But in the process the disease sickened more than 8,000 people in 29 countries and claimed 774 lives.
Because COVID-19 is more contagious, it has had a far greater impact, with more than 15 million cases worldwide, including 618,000 deaths.
“It is so efficient in its ability to transmit from human to human that I think we ultimately will get control of it. I don’t really see us eradicating it,” Fauci said.
President Trump has repeatedly said the virus will eventually disappear, even though that is rare for most infectious diseases.
Fauci, who is a member of the White House coronavirus task force, recently responded to Trump’s characterization of him as “a little bit of an alarmist” on the pandemic by saying he prefers to think of himself as “a realist.”
During Wednesday’s interview, Fauci described ways that the U.S. can get the coronavirus under control.
“I think with a good combination of good public health measures, a degree of global herd immunity and a good vaccine, which I do hope and feel cautiously optimistic we will get, I think when you put all three of those together we will get very good control of this. Whether it’s this year or next year, I’m not certain,” he added.
“We’ll bring it down to such a low level that we will not be in the position we are right now for an extended period of time.”
Why COVID-19’s biggest impact on healthcare may not be until 2022

This perfect storm of a shift in payer mix, the impending insolvency of Medicare and the inability of states to absorb the growing costs of Medicaid represent a tsunami of challenges.
With COVID-19 there has been unprecedented stress placed upon the healthcare system. The human and financial toll of the current crisis has been extraordinary. Yet, little attention has been focused on the impact of this virus on the viability of our healthcare financing system.
Three significant shifts in healthcare financing are occurring as a result of the pandemic’s economic impact. First, as a result of job losses, there will be a shift in commercial insurance to government-funded insurance programs. Second, revenue for funding Medicare, based on payroll taxes, will be significantly decreased. Finally, states will have less tax revenue to pay for Medicaid, threatening the viability of this program as well.
More than 30 million Americans have filed for unemployment since the start of the COVID-19 pandemic. According to a recent report, about 27 million people may lose their employer-sponsored insurance.
This will result in millions of people seeking coverage through Medicaid programs, the individual marketplace or simply becoming uninsured. Healthcare providers have relied upon margins from commercial insurance to offset costs from poorer reimbursing government funded programs and uncompensated care.
With more than 156 million Americans receiving employer sponsored insurance at the start of this year, and given recent projected job losses, providers may see a 17% shift in payer mix. The reliance on commercial insurance and cost shifting has become a necessary way for providers to financially sustain operations.
With a 35% margin with commercial insurance compared to Medicare, a 17% shift in payer mix on a trillion dollar spend would result in a substantial reduction in financial resources available to hospitals.
Almost half of healthcare expenditures already come from government programs. Medicare, the largest of these programs, is principally supported by taxes on payroll and social security benefits. With COVID-related job losses there will be a corresponding reduction in payroll tax revenues to the Medicare system. Reports from the Congressional Research Service submitted to Congress in May, with data used prior to COVID-19, projected that Medicare would become insolvent in 2026.
Analyses performed show that there will be a gap in Medicare revenues during the next three years (from the pre-COVID projections) of close to $150 billion. The result is that Medicare will become insolvent as early as 2022. Even by applying more conservative projections, such as recovering all job losses by the end of 2020 and payroll tax revenue holding steady at pre-COVID levels, Medicare still becomes insolvent in 2023.
State revenues, too, will be under real pressure with reduced tax revenues resulting from the current economic downturn. Medicaid programs are supported in part by federal funds, but also from general funds from the state.
On average, states are projecting about a 10% reduction in revenues in 2020, rising to almost a 25% reduction in 2021. Even without considering the growth in Medicaid enrollment hitting states, this reduced tax revenue will make sustaining current Medicaid program funding increasingly difficult.
This perfect storm of a shift in payer mix, the impending insolvency of Medicare by 2022 and the inability of states to absorb the growing costs of Medicaid represent a tsunami of challenges for the health system. Looking at this new reality, it is clear that our system for financing healthcare is severely broken and we must identify solutions to sustain access to medical care for our citizens.
This will be a challenge of a generation and we will need strength, courage and bold ideas to get through this. Pandemics have a way of changing a society’s political, economic and sociologic outlooks, and COVID-19 will be no different.
Is telehealth as good as in-person care?

COVID-19 has led to a boom in telehealth, with some health care facilities seeing an increase in its use by as much as 8,000%.
This shift happened quickly and unexpectedly and has left many people asking whether telehealth is really as good as in-person care.
Over the last decade, I’ve studied telehealth as a Ph.D. researcher while using it as a registered nurse and advanced practice nurse. Telehealth is the use of phone, video, internet and technology to perform health care, and when done right, it can be just as effective as in-person health care. But as many patients and health care professionals switch to telehealth for the first time, there will inevitably be a learning curve as people adapt to this new system.
So how does a patient or a provider make sure they are using telehealth in the right way? That is a question of the technology available, the patient’s medical situation and the risks of going – or not going – to a health care office.

Telehealth technologies
There are three main types of telehealth: synchronous, asynchronous and remote monitoring. Knowing when to use each one – and having the right technology on hand – is critical to using telehealth wisely.
Synchronous telehealth is a live, two-way interaction, usually over video or phone. Health care providers generally prefer video conferencing over phone calls because aside from tasks that require physical touch, nearly anything that can be done in person can be done over video. But some things, like the taking of blood samples, for example, simply cannot be done over video.
Many of the limitations of video conferencing can be overcome with the second telehealth approach, remote patient monitoring. Patients can use devices at home to get objective data that is automatically uploaded to health care providers. Devices exist to measure blood pressure, temperature, heart rhythms and many other aspects of health. These devices are great for getting reliable data that can show trends over time. Researchers have shown that remote monitoring approaches are as effective as – and in some cases better than – in-person care for many chronic conditions.
Some remaining gaps can be filled with the third type, asynchronous telehealth. Patients and providers can use the internet to answer questions, describe symptoms, refill prescription refills, make appointments and for other general communication.
Unfortunately, not every provider or patient has the technology or the experience to use live video conferencing or remote monitoring equipment. But even having all the available telehealth technology does not mean that telehealth can solve every problem.

Ongoing care and first evaluations
Generally, telehealth is right for patients who have ongoing conditions or who need an initial evaluation of a sudden illness.
Because telehealth makes it easier to have have frequent check-ins compared to in-person care, managing ongoing care for chronic illnesses like diabetes, heart disease and lung disease can be as safe as or better than in-person care.
Research has shown that it can also be used effectively to diagnose and even treat new and short-term health issues as well. The tricky part is knowing which situations can be dealt with remotely.
Imagine you took a fall and want to get medical advice to make sure you didn’t break your arm. If you were to go to a hospital or clinic, almost always, the first health care professional you’d see is a primary care generalist, like me. That person will, if possible, diagnose the problem and give you basic medical advice: “You’ve got a large bruise, but nothing appears to be broken. Just rest, put some ice on it and take a pain reliever.” If I look at your arm and think you need more involved care, I would recommend the next steps you should take: “Your arm looks like it might be fractured. Let’s order you an X-ray.”
This first interaction can easily be done from home using telehealth. If a patient needs further care, they would simply leave home to get it after meeting with me via video. If they don’t need further care, then telehealth just saved a lot of time and hassle for the patient.
Research has shown that using telehealth for things like minor injuries, stomach pains and nausea provides the same level of care as in-person medicine and reduces unnecessary ambulance rides and hospital visits.
Some research has shown that telehealth is not as effective as in-person care at diagnosing the causes of sore throats and respiratory infections. Especially now during the coronavirus pandemic, in-person care might be necessary if you are having respiratory issues.
And finally, for obviously life-threatening situations like severe bleeding, chest pain or shortness of breath, patients should still go to hospitals and emergency rooms.

Balancing risk
With the right technology and in the right situations, telehealth is an incredibly effective tool. But the question of when to use telehealth must also take into account the risk and burden of getting care.
COVID-19 increases the risks of in-person care, so while you should obviously still go to a hospital if you think you may be having a heart attack, right now, it might be better to have a telehealth consultation about acne – even if you might prefer an in-person appointment.
Burden is another thing to consider. Time off work, travel, wait times and the many other inconveniences that go along with an in-person visit aren’t necessary simply to get refills for ongoing medication. But, if a provider needs to draw a patient’s blood to monitor the safety or effectiveness of a prescription medicine, the burden of an in-person visit to the lab is likely worth the increased risk.
Of course, not all health care can be done by telehealth, but a lot can, and research shows that in many cases, it’s just as good as in-person care. As the pandemic continues and other problems need addressing, think about the right telehealth fit for you, and talk to your health care team about the services offered, your risks and your preferences. You might find that that there are far fewer waiting rooms in your future.
New unemployment insurance claims rise for the first time since March

Some 1.4 million workers filed for unemployment last week, the first increase in months, as the pandemic continues to weigh on the labor market
“What you’re seeing is that, as the economy slows, the pace of claims picks back up — which really puts at risk the monthly jobs report over the next few months,” said Joseph Brusuelas, the chief economist at RSM. “The July numbers are going to be tenuous, but it’s August that I’m worried about.”
The number of workers continually claiming unemployment insurance went down, however, a statistic that lags by a week, to 16.1 million workers for the week ending July 11, from 17.4 million for the week ending July 4.
In addition to the 1.4 million seeking unemployment nationwide last week, another 980,000 new Pandemic Unemployment Assistance claims were filed, the benefits offered to self-employed and gig workers.
The numbers come as millions of unemployed workers are about to exhaust stimulus payments from two federal benefits programs whose expiration economists have warned could have dire effects on the economy.
Brusuelas said the numbers are a sign that the burst of economic activity that marked the country’s reopening has waned, and that shrinking consumer demand remained a significant risk for businesses and the workers they employ across the country.
“We are going to see a much slower pace of growth the reset of the year,” he said. “While we still are retaining our call for a swoosh-shaped recovery, one has to acknowledge a w-shaped recovery is possible.”
The extra $600 a week in unemployment benefits that the federal government has offered to supplement more modest state unemployment benefits will end this week, as lawmakers wrangle over legislation that could extend it.
Including the new benefits available to gig workers and the self-employed, more than 53 million applications have been filed for some form of unemployment insurance during the pandemic.
Cartoon – Pandemic Management
Will Telemedicine Be the Blockbuster or Netflix of Healthcare?

New approaches need to recognize patients’ wants and needs
One component of Blockbuster’s financial model was the late fees it charged to customers who did not return a video tape to the store in time. These fees accounted for up to 16% of its revenue. In 1997, Reed Hastings was one of the customers affected by these fees. After one late rental, he was charged a hefty $40 late fee. His frustration inspired him to help create a company that would have no late charges. This new company also had the audacious idea to send DVDs straight to the customer’s home for a flat monthly fee. The company that Reed Hastings co-founded was Netflix.
Over time, Netflix changed and adapted with new technology and shifting consumer preferences. It moved on from mailing DVDs to using a streaming platform. It developed an algorithm to help make personalized video recommendations to Netflix users. It started producing its own video content. Over time, the company planted itself firmly within many homes and routines. Conversely, Blockbuster adapted to new platforms too slowly and too late. After its peak in 2004, Blockbuster started losing market share and relevance. Today, there is only one Blockbuster store left, a curious tourist attraction in Bend, Oregon.
Markets and industries change all the time. Distinguishing these important changes from temporary fads is essential. History has many examples of companies and organizations that did not sense important changes, did not change their approach, and as a result, ended up obsolete and irrelevant. A similar shift is happening today in healthcare, but there is more at stake than a late fee. Like Netflix, the healthcare industry needs to shift and adapt to consumer preferences.
The COVID-19 pandemic has had an immediate impact on the health of our country and has also indelibly changed how patients interact with the healthcare system. Hospitals and providers around the country have had to quickly develop new strategies to connect with patients – to comply with social distancing guidelines, in an effort to slow down the spread of the virus. Consistent communication and accessibility is vital, especially given the disturbing trends in decreased preventive care visits and delayed emergency care. One solution is telehealth.
During this pandemic, we have seen that remote patient monitoring is valuable for patients with a wide variety of needs: certainly, those quarantined with coronavirus, but for healthy patients too – children in need of regularly scheduled well-child visits and adults who need routine care. Many patients have experienced telehealth for the first time and many have positive impressions, with nearly three quarters of patients who had a recent telehealth visit describing it as good or very good, according to a recent survey.
Even after the COVID-19 pandemic settles, these “temporary” approaches will permanently change patient attitudes towards technology and force healthcare providers to reexamine their approach to care. Telehealth will remain a convenient option and, in some cases, a necessary way to receive care. Embedding telehealth into standard practice of care enables providers to expand the access to people who otherwise might forgo care, and to people who may face barriers getting to a clinic, for example patients with inflexible job schedules or limited transportation.
Patients and providers are not the only people recognizing the benefits; government officials are too. While reimbursement rules were temporarily expanded to include telehealth, some states, such as Colorado and Idaho, are making COVID-19 telehealth expansions permanent.
There are many parallels to borrow from the Blockbuster example. As healthcare providers, we cannot be complacent and stick with old business models because they are what we are used to. We cannot wait for people to come to us. We cannot ignore these changing times and consumers’ changing preferences. In fact, if we adapt and provide care in ways that patients prefer, we could improve health outcomes.
The healthcare institutions that will grow and be successful during this time are those who are more like Netflix. Instead of waiting for patients to decide to seek healthcare when it may be too late (e.g., just like a Blockbuster “late fee”), we will actively reach out and remind our patients about the importance of timely healthcare services. Instead of ignoring changes in patient preferences and new technology, we will adapt quickly to new platforms for healthcare visits. Instead of waiting for patients to feel comfortable to return to a healthcare facility, we will show patients what our healthcare system is doing to ensure patient safety and protection from COVID-19. Most importantly, instead of being complacent, we will accept and develop new ways of providing care.
There was once a time that we thought that getting in a car, driving to a strip mall, and walking through aisles with thousands of video tapes was the only option to watch a movie at home. Now, many of us can get thousands of titles on our televisions, computers, and phones through several movie streaming platforms. The COVID-19 pandemic has forced healthcare systems to quickly adapt to new constraints; however, it may really be an opportunity to develop new models of care, to engage with our patients, and to make healthcare more accessible. As healthcare providers, we need to make the choice to be more like Netflix, and less like Blockbuster.

The Constitution doesn’t have a problem with mask mandates

Many public health professionals and politicians are urging or requiring citizens to wear face masks to help slow the spread of the COVID-19 virus.
Some Americans have refused, wrongly claiming mask decrees violate the Constitution. An internet search turns up dozens of examples.
“Costco Karen,” for instance, staged a sit-in in a Costco entrance in Hillsboro, Oregon after she refused to wear a mask, yelling “I am an American … I have rights.”
A group called Health Freedom Idaho organized a protest against a Boise, Idaho, mask mandate. One protester said, “I’m afraid where this country is headed if we just all roll over and abide by control that goes against our constitutional rights.”
As one protester said, “The coronavirus doesn’t override the Constitution.”
Speaking as a constitutional law scholar, these objections are nonsense.

The objections
It is not always clear why anti-maskers think government orders requiring face coverings in public spaces or those put in place by private businesses violate their constitutional rights, much less what they think those rights are. But most of the mistaken objections fall into two categories:
Mandatory masks violate the First Amendment right to speech, assembly, and especially association and mandatory masks violate a person’s constitutional right to liberty and to make decisions about how to their own health and bodily integrity.
They’re not mutually exclusive claims: A lawsuit filed by four Florida residents against Palm Beach County, for example, argues that mask mandates “interfere with … personal liberty and constitutional rights,” such as freedom of speech, right to privacy, due process, and the “constitutionally protected right to enjoy and defend life and liberty.” The lawsuit asks the court to issue a permanent injunction against the county’s mask mandate.
Responding to a reporter who asked why President Donald Trump appeared unconcerned about the absence of masks and social distancing at a campaign rally in Tulsa, Vice President Mike Pence said: “I want to remind you again freedom of speech and the right to peaceably assemble is in the Constitution of the U.S. Even in a health crisis, the American people don’t forfeit our constitutional rights.”
What the First Amendment does – and doesn’t – do
The First Amendment protects freedom of speech, press, petition, assembly and religion.
There are two reasons why mask mandates don’t violate the First Amendment.
First, a mask doesn’t keep you from expressing yourself. At most, it limits where and how you can speak. Constitutional law scholars and judges call these “time, place, and manner” restrictions. If they do not discriminate on the basis of the content of the speech, such restrictions do not violate the First Amendment. An example of a valid time, place and manner restriction would be a law that limits political campaigning within a certain distance of a voting booth.
Additionally, the First Amendment, like all liberties ensured by the Constitution, is not absolute.
All constitutional rights are subject to the goverment’s authority to protect the health, safety and welfare of the community. This authority is called the “police power.” The Supreme Court has long held that protecting public health is sufficient reason to institute measures that might otherwise violate the First Amendment or other provisions in the Bill of Rights. In 1944, in the case of Prince v. Massachusetts, for example, the Supreme Court upheld a law that prohibited parents from using their children to distribute religious pamphlets on public streets.
The right to liberty
Some anti-maskers object that masks violate the right to liberty.
The right to liberty, including the right to make choices about one’s health and body, is essentially a constitutional principle of individual autonomy, neatly summarized as “My body, my choice.”
The 1905 case of Jacobsen v. Massachusetts shows why mask mandates don’t violate any constitutional right to privacy or health or bodily integrity. In that case, the Supreme Court upheld a smallpox vaccination requirement in Cambridge, Massachusetts.
The court said that the vaccination requirement did not violate Jacobsen’s right to liberty or “the inherent right of every freeman to care for his own body and health in such way as to him seems best.”
As the court wrote, “There are manifold restraints to which every person is necessarily subject for the common good. On any other basis, organized society could not exist with safety to its members.” In a 1995 New York case, a state court held that an individual with active tuberculosis could be forcibly detained in a hospital for appropriate medical treatment.
Even if you assume that mask mandates infringe upon what the Supreme Court calls “fundamental rights,” or rights that the court has called the “very essence of a scheme of ordered liberty,” it has consistently ruled states can act if the restrictions advance a compelling state interest and do so in the least restrictive manner.
Rights are conditional
As the Jacobsen ruling and the doctrine of time, place and manner make clear, the protection of all constitutional liberties rides upon certain necessary – but rarely examined – assumptions about communal and public life.
One is that is constitutional rights – whether to liberty, speech, assembly, freedom of movement or autonomy – are held on several conditions. The most basic and important of these conditions is that our exercise of rights must not endanger others (and in so doing violate their rights) or the public welfare. This is simply another version of the police power doctrine.
Unfortunately, a global pandemic in which a serious and deadly communicable disease can be transmitted by asymptomatic carriers upsets that background and justifies a wide range of reasonable restrictions on our liberties. Believing otherwise makes the Constitution a suicide pact – and not just metaphorically.
