What role should the federal government play in addressing major healthcare issues? And does the way you vote affect your prospects for a long and healthy life? We talked about it on today’s episode of the 4sight Friday Roundup podcast.
David Johnson is CEO of 4sight Health.
Julie Vaughan Murchinson is Partner of Transformation Capital and former CEO of Health Evolution.
David Burda is News Editor and Columnist of 4sight Health.
Social factors impact a person’s health and their potential health outcomes. While this has long been discussed (especially by folks of color, individuals with lived experiences, and those in public health), it is finally now getting deserved mainstream attention, including by health insurers.
Medicare Advantage (MA) — a program that offers private plan alternatives to traditional Medicare — is one key player looking at social determinants of health. It’s a good thing, too; an estimated 42% of the Medicare population are enrolled in MA plans, and that share grows each year. MA plans have more flexibility in offering supplemental benefits and services, some of which can address social determinants of health.
In 2018, the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act passed with bipartisan support and marked a substantial shift in MA policy by including acknowledgment of the role of social determinants of health. It allows even greater flexibility for MA plans to help with the very conditions that impact how a person lives, such as providing financial assistance for nutritional needs, transportation to appointments, caregiver support, and even home construction projects. Interestingly, it does not mandate coverage, so it is still dependent on what plans an individual has access to and how health plans are choosing to move forward with this freedom.
The problem is, however, that most individuals aren’t eligible for Medicare until age 65 (there are some exceptions). If we wait until Medicare eligibility to act on social determinants of health, are we waiting too long?
The short answer is yes. Although addressing social determinants of health in the Medicare-eligible population is important, what we know suggests that more could be done earlier.
Why are social determinants important in Medicare Advantage?
Chronic disease is a significant issue among Medicare-eligible individuals, and one that’s exacerbated by social determinants of health. There are substantial implications for both beneficiaries and MA plans. For beneficiaries, chronic disease affects not only their quality of life, but also their wallet. From the plans’ perspectives, the presence of comorbid chronic diseases is a significant differentiator between so called “high cost” beneficiaries and those who are not.
Current MA enrollment trends also point to the need to sharpen the focus on social determinants of health. Although they make up a minority of MA enrollees, persons of color are enrolling in MA plans at a breakneck pace: especially among Black people, dual enrollees, and people living in disadvantaged neighborhoods.
Historically, these are folks most negatively impacted by social determinants of health, and the likelihood of poor health outcomes is only compounded when enrollees reside in disadvantaged neighborhoods. These are neighborhoods commonly characterized by high concentrations of poverty, crime, and harmful environmental exposures compounded by limited resources to support economic and social well-being, and research has consistently found strong associations between neighborhood disadvantage and health risks and outcomes.
Health systems must do more about social determinants earlier in life
Social determinants of health affect us all — regardless of age. Until recently, they have received relatively little attention from insurers.
It is difficult though to discern the extent that these actions are altruistic or opportunistic, especially when they can technically be both. While that might not be the worst thing, it does matter if it leaves out the very people it should be helping.
Let’s consider internet access, for example. If a patient isn’t connected to the web, they can’t participate in a telehealth visit, leaving in-person care as the only option. In a world where telehealth visits are reimbursed at a fraction of the in-person rate, there are substantial cost savings (read: profit) associated with facilitating and promoting virtual care. Critics have also pointed out that most of these steps can be attributed to insurers’ philanthropic apparatuses as opposed to any substantive change or innovation in member benefits.
What is also becoming readily apparent, is that while telehealth use is increasing, it does not make care accessible for everyone. It could even serve to increase disparities if it is not done properly.
However, administrative hurdles and societal stigma can challenge people’s willingness to participate in these programs no matter how beneficial they might be. We should all be asking what more the health system — providers, payers, and government — should be doing to improve social determinants of health earlier in life.
The CHRONIC Care Act has the potential to mitigate some of these harmful impacts of long-standing structural inequities by providing greater flexibility for plans to cover non-medical needs. The law illustrates that policymakers believe that health insurers should do more to address social determinants of health. Perhaps they should also focus on how plans can address these social factors earlier in the life cycle as well.
The momentum behind Medicare Advantage is only growing as more baby boomers age into eligibility, and experts don’t expect the energy around the program to slow down any time soon.
A recent analysis from the Kaiser Family Foundation found that a record 3,834 plans were available for the 2022 plan year in MA, which represents an 8% increase over 2021 and the largest number on the market in a decade.
Open enrollment for Medicare ended Dec. 7, and enrollment numbers will begin trickling out as the year winds down. In 2021, 26 million Medicare beneficiaries, or about 42% of those eligible for the program, were enrolled in an MA plan.
“As Medicare Advantage enrollment continues to grow, insurers seem to be responding by offering more plans and choices to the people on Medicare,” the KFF analysts said.
Part of the appeal of MA to an increasingly savvy consumer base is that it offers additional benefits beyond those afforded people in traditional Medicare, such as vision and dental coverage as well as supports for members’ social needs.
Sachin Jain, M.D., CEO of SCAN Health Plan, told Fierce Healthcare that people are increasingly shopping around for plans, building greater awareness of MA as a whole as well as of the different types of benefits beneficiaries could select.
“We’re seeing that consumers are more sophisticated today than they were a decade ago,” he said. “I think people are realizing that fee-for-service Medicare doesn’t cover a lot of things.”
The KFF report shows that more than 90% of non-group MA plans offer some kind of vision, hearing, telehealth or dental benefits and that most (89%) include prescription drug coverage as well.
Elena McFann, president of Medicare at Anthem, told Fierce Healthcare that throughout the open enrollment period, plans built with benefits that target the social determinants of health and promote whole-person care resonated strongly with members.
Anthem, for example, offers plans that include a slate of essential extra benefits that members can choose from based on what they need the most. Options include grocery cards, transportation benefits and in-home supports.
She said that the grocery benefits and flex cards that allow members to purchase additional hearing, vision and dental coverage have proven particularly popular in this enrollment season.
“What those all point to is the concept of flexibility and helping them lead healthier lives where they really need the help where they are in their journey,” McFann said.
As these benefits prove popular, an increasing number of plans are offering them in tandem. The Better Medicare Alliance released a survey late last month that found the number of plans including supplemental benefits grew by 43% for the 2022 plan year.
The Centers for Medicare & Medicaid Services (CMS) has issued additional flexibilities that allow MA plans to address members’ social determinants of health as the program’s enrollment continues to swell.
Jain said SCAN has seen similar interest in supplemental benefits, and that flexibility afforded to MA plans to adapt to seniors’ needs and expectations is a critical factor in the program’s success.
“When you’re in the business of serving seniors, a lot of what you have to do is anticipate needs that those seniors may not anticipate that they have, give them things they didn’t know they needed,” he said.
McFann said that beneficiaries value plans like these that unite brands they trust and recognize and that partners like Kroger enable insurers to more effectively meet seniors where they are. In its co-branded plans, members can access benefits like Healthy Grocery Cards and stipends to purchase over-the-counter health items.
She said that there has been significant “excitement” around those plans, which are available in four states, during the current enrollment period.
“It gives the Medicare eligibles a sense of familiarity and a sense of comfort, again meeting them on their terms,” McFann said.
However, while many established insurers have set ambitious growth targets in this market and new startups enter the space regularly, they still have plenty of work to do if they want to catch up with the market’s dominant forces: UnitedHealthcare, Humana and Blues plans.
UHC and Humana together account for 45% of the MA market in 2021, according to the KFF analysis. Humana offers plans in 85% of counties and UHC in 74% for 2022.
That means, 89% of Medicare eligibles have access to a Humana plan and 90% have access to a UHC MA plan if they choose, according to the report.
Competition is continuing to grow, though, and both McFann and Jain said they don’t feel the momentum around MA slowing down anytime soon.
“It is those extras and social drivers of health solutions that really have caught on with the Medicare-eligible segment and we expect to see that expand even further,” McFann said.
Welcome to Friday’s Health 202, where today we have a special spotlight on the pandemic two years in.
🚨 The federal government is about to be funded. The Senate sent the long-term spending bill to President Biden’s desk last night after months of intense negotiations.
Two years since the WHO declared a pandemic, what health-care system changes are here to stay?
Nurses screened patients at a drive-through testing site in March 2020. (Win McNamee/Getty Images)
Exactly two years ago, the World Health Organizationdeclared the coronavirus a pandemic and much of American life began grinding to a halt.
That’s when the health-care system, which has never been known for its quickness, sped up. The industry was forced to adapt, delivering virtual care and services outside of hospitals on the fly. Yet, the years-long pandemic has exposed decades-old cracks in the system, and galvanized efforts to fix them.
Today, as coronavirus cases plummet and President Biden says Americans can begin resuming their normal lives, we explore how the pandemic could fundamentally alter the health-care system for good. What changes are here to stay — and what barriers are standing in the way?
A telehealth boom
What happened: Telehealth services skyrocketed as doctors’ offices limited in-person visits amid the pandemic. The official declaration of a public health emergency eased long-standing restrictions on these virtual services, vastly expanding Medicare coverage.
But will it stick? Some of these changes go away whenever the Biden administration decides not to renew the public health emergency (PHE). The government funding bill passed yesterday extends key services roughly five months after the PHE ends, such as letting those on Medicare access telehealth services even if they live outside a rural area.
But some lobbyists and lawmakers are pushing hard to make such changes permanent. Though the issue is bipartisan and popular, it could be challenging to pass unless the measures are attached to a must-pass piece of legislation.
“Even just talking to colleagues, I used to have to spend three or four minutes while they were trying desperately not to stare at their phone and explain to them what telehealth was … remote patient monitoring, originating sites, and all this wonky stuff,”said Sen. Brian Schatz (D-Hawaii), a longtime proponent of telehealth.
“Now I can go up to them and say, ‘So telehealth is great, right?’ And they say, ‘yes, it is.’ ”
A new spotlight on in-home care
What happened: The infectious virus tore through nursing homes, where often fragile residents share rooms and depend on caregivers for daily tasks. Ultimately, nearly 152,000 residents died from covid-19.
The devastation has sparked a rethinking of where older adults live and how they get the services they need — particularly inside their own homes.
“That is clearly what people prefer,” said Gail Wilensky, an economist at Project HOPE who directed the Medicare and Medicaid programs under President George H.W. Bush. “The challenge is whether or not it’s economically feasible to have that happen.”
More money, please: Finding in-home care — and paying for it — is still a struggle for many Americans. Meanwhile, many states have lengthy waitlists for such services under Medicaid.
Experts say an infusion of federal funds is needed to give seniors and those with disabilities more options for care outside of nursing homes and assisted-living facilities.
For instance, Biden’s massive social spending bill included tens of billions of dollars for such services. But the effort has languished on Capitol Hill, making it unclear when and whether additional investments will come.
A reckoning on racial disparities
What happened: Hispanic, Black, and American Indian and Alaska Native people are about twice as likely to die from covid-19 than White people. That’s according to age-adjusted data from a recent Kaiser Family Foundation report.
In short, the coronavirus exposed the glaring inequities in the health-care system.
“The first thing to deal with any problem is awareness,” said Georges Benjamin, the executive director of the American Public Health Association. “Nobody can say that they’re not aware of it anymore, that it doesn’t exist.”
But will change come? Health experts say they hope the country has reached a tipping point in the last two years. And yet, any real systemic change will likely take time. But, Benjamin said, it can start with increasing the number of practitioners from diverse communities, making office practices more welcoming and understanding biases.
We need to, as a matter of course, ask ourselves who’s advantaged and who’s disadvantaged” when crafting new initiatives, like drive-through testing sites, Benjamin said. “And then how do we create systems so that the people that are disadvantaged have the same opportunity.”
The agency’s end goal for Medicare Advantage is to match CMS’ vision for its programs as a whole, with an emphasis on health equity.
On Wednesday, the Centers for Medicare and Medicaid Services released proposed payment policy changes for Medicare Advantage and Part D drug programs in 2023 that are meant to create more choices and provide affordable options for consumers.
The Calendar Year 2023 Advance Notice for Medicare Advantage and Part D plans is open to public comment for 30 days. This year, CMS is soliciting input through a health equity lens on the approach to some future potential changes.
The agency’s end goal for Medicare Advantage is to match CMS’ vision for its programs as a whole, which Administrator Chiquita Brooks-LaSure said is “to advance health equity; drive comprehensive, person-centered care; and promote affordability and the sustainability of the Medicare program.”
CMS is proposing an effective growth rate of 4.75% and an overall expected average change in revenue of 7.98%, following a 4.08% revenue increase planned for 2022.
WHAT’S THE IMPACT?
CMS is requesting input on a potential change to the MA and Part D Star Ratings that would take into account how well each plan advances health equity.
The agency is also requesting comment on including a quality measure in MA and Part D Star Ratings that would assess how often plans are screening for common health-related social needs, such as food insecurity, housing insecurity and transportation problems.
The Health Equity Index has been tasked with creating more transparency on how MA plans care for disadvantaged beneficiaries.
Additionally, CMS is requesting input on considerations for assessing the impact of using sub-state geographic levels of rate setting for enrollees with end-stage renal disease, particularly input regarding the impact of MA payment on care provided to rural and urban underserved populations and how such payment changes may impact health equity.
Other areas in which CMS is soliciting input include a variety of payment updates, a new measure concept to assess whether and how MA plans are transforming care by engaging in value-based models with providers’ and updates to risk-adjustment models to continue to pay appropriately for people enrolled in MA and Part D plans.
Public comments on the Advance Notice must be submitted by March 4. The Medicare Advantage and Part D payment policies for 2023 will be finalized in the 2023 Rate Announcement, which will be published no later than April 4.
REACTION
The proposed rule has already elicited reaction from various organizations, including Better Medicare Alliance.
“As we continue to review the Advance Notice in further detail, we appreciate that CMS has offered a thoughtful proposal that will help ensure stability for the millions of diverse seniors and individuals with disabilities who count on Medicare Advantage,” Mary Beth Donahue, president and CEO of the Better Medicare Alliance, said, adding that the proposal furthers the shared goal of improving health equity.
“Medicare Advantage has proven its worth for seniors and taxpayers – providing lower costs, meaningful benefits that address social determinants of health, better outcomes and greater efficiencies for the Medicare dollar,” she said. “A stable rate for 2023 ensures this work can continue. On behalf of our 170 Ally organizations and over 600,000 beneficiary advocates, we applaud CMS for putting seniors first by issuing an Advance Notice that protects coverage choices, advances health equity and preserves affordability for beneficiaries.”
AHIP also responded, with President and CEO Matt Eyles pointing out that for 2022 the average Medicare Advantage monthly premium dropped to $19, down more than 10% since 2021.
“We agree that MA plans play an essential role in improving health equity and addressing the social determinants of health that impact millions of seniors and people with disabilities,” he said. “We support CMS soliciting input on ways to advance these important goals.
“Medicare Advantage enjoys strong bipartisan support because it provides America’s seniors and people with disabilities with access to affordable, high-quality healthcare services,” said Eyles. “We will continue to review the 2023 rate notice and look forward to providing constructive feedback to CMS during the comment period.”
THE LARGER TREND
CMS’ Advance Notice follows a recent congressional letter in which 346 bipartisan members of Congress declared support for Medicare Advantage and urged the agency “to provide a stable rate and policy environment” for the program in 2023.
A December 2021 Morning Consult poll showed that 94% of Medicare Advantage beneficiaries are satisfied with their coverage, while 93% believe that protecting MA should be a priority of the Biden administration.
Massachusetts-based health system Wellforce recently appointed its first ever chief consumer officer, tapping an executive from a well-known sneaker brand.
Christine Madigan joined the health system to lead marketing and consumer engagement, Wellforce announced in January. She comes from New Balance Athletics, where she led the global marketing and brand management organization. Madigan was attracted to what she termed the “challenger brand” because of its nimble innovation strategy and its mission to help people live healthier. “I can’t imagine a more purpose-driven culture than that,” she told Fierce Healthcare.
“As a marketing veteran from consumer products, Christine understands the importance of envisioning and building services around consumer needs. She will be a great asset in improving and modernizing the way consumers engage with the health care industry,” David Storto, Wellforce’s executive vice president and chief strategy and growth officer, said in the announcement.
The move comes amid a rising trend in healthcare: executives sourced from outside the industry, and in particular from consumer brands, to lead innovation strategies. Fierce Healthcare spoke to several, some of whom have been in their roles for years. They agree that while there are many transferrable skills, there is also an advantage to being an outsider.
To Madigan, the core challenge remains the same business to business—understanding who the consumer is and the different ways they engage with one’s brand.
Aaron Martin, chief digital officer at Providence St. Joseph Health, who joined the health system from Amazon in 2016, echoed Madigan. “Bringing the patient focus—what we called at Amazon ‘customer obsession’—to Providence was key,” he told Fierce Healthcare.
Society is bombarded by healthcare marketing messages, Madigan noted. She wants to “drive some simplicity into the process.” While the system is built to provide reactive, acute care, Madigan sees preventive care as just as important. And a crucial part of facilitating that is establishing not only awareness of but trust in a provider. “Every detail matters in what you communicate in an experience,” she said.
And for organizations that don’t innovate, “somebody else is going to disrupt us,” Martin said.
To drive innovation at scale, Martin sees a disciplined strategy as key. At Amazon, that looked like picking an area to impact and measuring the value of closing that gap. Applying that to Providence, Martin worked with the clinical team to discover patients in need of low-acuity care were going to other providers instead of to Providence. So Providence launched ExpressCare, offering virtual appointments to recapture those patients and establish continuity of care.
Like Madigan, Novant’s chief digital and transformation officer Angela Yochem, who has held chief information officer roles at Rent-A-Center and BDP International, believes passive care is not enough to eradicate health inequities. “We’ve optimized for fixing things,” she said of the healthcare system. “I’d like to see the healthcare industry become more engaged continually. We need to understand our patients beyond what their last condition is,” she added, referring to social determinants of health.
“In retail, we used to say that customers shouldn’t have to shop our merchandising organizational chart,” said Prat Vemana, Kaiser Permanente’s chief digital officer, who transitioned in 2019 from chief product and experience officer at The Home Depot. To streamline how patients navigate an already highly fragmented healthcare system, Kaiser starts with the patient and works backward when developing digital experiences.
A challenge in healthcare, Vemana acknowledged, is the lag in data around health outcomes. Whereas in retail, results are immediately visible, healthcare is less straightforward. “We have to develop workarounds to get directional information while waiting to see the results,” he said.
The transformation of the sector won’t happen without diversity of thought and experience, Yochem said. It’s less about hiring from a particular sector and more about hiring from all over. Those people will have seen the potential for consumer engagement and will be able to “apply what we know to be possible,” Yochem said. Without those outsider insights in the insular sector, “you create an echo chamber, because you respond to problems in the same way.”
The COVID-19 pandemic revealed the need for substantial investment in public health. Journalist Anna Maria Barry-Jester, in an investigation published in California Healthline and the Los Angeles Times last week, reported that the need is pressing and that the time is ripe to formulate solutions.
“As we’ve continued to make progress in bringing the COVID-19 emergency under control, many California leaders are turning their attention to the future,” Barry-Jester wrote.
This year’s state budget set aside $3 million for an assessment of California’s public health infrastructure. “Public health leaders believe it will show that staffing and training are major issues,” Barry-Jester reported.
Starting in July 2022, annual state budgets will include $300 million to be spent to improve public health infrastructure.
The pandemic highlighted two significant public health needs in California. One is basic investment in public health infrastructure, as highlighted by Barry-Jester. The other is to address housing, diet, livable wages, and access to quality health care as part of an overarching public health strategy — a necessity highlighted by the stark racial, ethnic, and economic disparities among those who contracted and died from COVID-19.
Many Reasons for Staff Attrition
Before the pandemic, the state’s public health infrastructure already required shoring up. The COVID-19 crisis hammered the already underfunded and understaffed county and state public health systems.
In California, public health workers are leaving their jobs in droves. Counties are “losing experienced staffers to retirement, exhaustion, partisan politics, and higher-paying jobs,” Barry-Jester reported.
The exodus from public health predated this surge of resignations. Since the early days of the pandemic, experienced California public health leaders have been leaving the field, including 17 county public health officers and 27 county-level directors or assistant directors of public health. Both the director and the deputy director of the state’s department of public health resigned during the pandemic.
“Public health nurses, microbiologists, epidemiologists, health officers, and other staff members who fend off infectious diseases like tuberculosis and HIV, inspect restaurants, and work to keep communities healthy are abandoning the field,” Barry-Jester wrote. “The collective expertise lost with those departures is hard to overstate.”
Public health laboratories illustrate how much we rely on public health infrastructure for our everyday safety. The labs are largely invisible to the public but touch every aspect of daily life. “Public health labs sample shellfish to make sure it is safe for eating. They monitor drinking water and develop tests for emerging health threats such as antibiotic-resistant viruses. They also test for serious diseases, such as measles and COVID-19. And they typically do it at a fraction of the cost of commercial labs — and faster.”
Yet labs across the state are unable to hire and retain staff, and they are in danger of closing. “The biggest threat to [public health labs] right now is not the next emerging pathogen,” said Donna Ferguson, director of the public health lab in Monterey County, “but labs closing due to lack of staffing.”
Addressing Social Needs as Public Health Strategy
The pandemic highlighted the effects of income inequality and racial disparitieson health in California. Data from the California Department of Public Health highlight the stark disparities in COVID-19 outcomes. The COVID-19 death rate for Latinx people is 19% higher than the statewide death rate, and the death rate for Black people is 16% higher. The case rate for Pacific Islanders is 45% higher than the statewide rate, while the rate of Pacific Islanders earning less than $40,000 annually is 33% higher than average.
“There is an 80% higher rate of diabetes among Hispanics compared to non-Hispanic whites. We think early life nutrition is very important but also the environment where people live, which can include a combination of factors like poor access to healthy food, poor access to resources, air pollution, even chemical contaminants in the environment we found contribute to this disparity,” he told Los Angeles Times reporter Alejandra Reyes-Velarde.
These chronic diseases then put Latinx people at higher risk for worse COVID outcomes. “One of the most common recurring risk factors, not so much for rates of infection but the severity of the infection, is blood-glucose levels,” he said. “Individuals with higher blood-glucose levels seem to have a more severe response to COVID-19 infection, and of course, higher blood glucose is what contributes to diabetes.”
A Health Affairs study from the early days of the pandemic, which drew on data from California’s Sutter hospitals, noted that Black people are similarly at higher risk from the chronic illnesses that make people more susceptible to poor outcomes from COVID infections, including type 2 diabetes and congestive heart failure, as do other populations disproportionately harmed by COVID-19.
“Already underfunded and neglected even before the pandemic, public health has been further undermined in ways that could resound for decades to come,” wrote journalists Mike Baker and Danielle Ivory. The Times investigation of hundreds of health departments in all 50 states revealed that “local public health across the country is less equipped to confront a pandemic now than it was at the beginning of 2020.”
Threats, harassment, and anger directed at public health officials and workers drove many out of the field since the beginning of the pandemic and was identified as an ongoing problem by Baker and Ivory. “We have learned all the wrong lessons from the pandemic,” Adriane Casalotti told them. Casalotti is the chief of public and government affairs for the National Association of County and City Health Officials, an organization representing the nearly 3,000 local health departments across the nation. “We are attacking and removing authority from the people who are trying to protect us.”
Officials interviewed by Baker and Ivory noted that while additional funds are crucial to rebuilding public health departments, they aren’t sufficient to address the problems that have long weighed down the system or those that emerged during the pandemic.
Melissa Lyon, public health director for Erie County, Pennsylvania, put it this way: “If a ship is sinking, throwing treasure chests of gold at the ship is not going to help it float.”
Health economists study the economic determinants of health. They also analyze how health care resources are utilized and allocated, and how health care policies and quality of care can be improved. In this episode, we discuss what exactly a healthcare system would look like if these professionals were calling all the shots.
At a certain point, it was no longer a matter of if the United States would reach the gruesome milestone of 1 in 500 people dying of covid-19, but a matter of when. A year? Maybe 15 months? The answer: 19 months.
Given the mortality rate from covid and our nation’s population size, “we’re kind of where we predicted we would be with completely uncontrolled spread of infection,” said Jeffrey D. Klausner, clinical professor of medicine, population and public health sciences at the University of Southern California’s Keck School of Medicine. “Remember at the very beginning, which we don’t hear about anymore, it was all about flatten the curve.”
The idea, he said, was to prevent “the humanitarian disaster” that occurred in New York City, where ambulance sirens were a constant as hospitals were overwhelmed and mortuaries needed mobile units to handle the additional dead.
The goal of testing, mask-wearing, keeping six feet apart and limiting gatherings was to slow the spread of the highly infectious virus until a vaccine could stamp it out. The vaccines came but not enough people have been immunized, and the triumph of science waned as mass death and disease remain. The result: As the nation’s covid death toll exceeded 663,000 this week, it meant roughly 1 in every 500 Americans had succumbed to the disease caused by the coronavirus.
While covid’s death toll overwhelms the imagination, even more stunning is the deadly efficiency with which it has targeted Black, Latino, and American Indian and Alaska Native people in their 30s, 40s and 50s.
Death at a younger age represents more lost years of life. Lost potential. Lost scholarship. Lost mentorship. Lost earnings. Lost love.
Neighborhoods decimated. Families destroyed.
“So often when we think about the majority of the country who have lost people to covid-19, we think about the elders that have been lost, not necessarily younger people,” said Abigail Echo-Hawk, executive vice president at the Seattle Indian Health Board and director of the Urban Indian Health Institute. “Unfortunately, this is not my reality nor that of the Native community. I lost cousins and fathers and tribal leaders. People that were so integral to building up our community, which has already been struggling for centuries against all these things that created the perfect environment for covid-19 to kill us.”
Six of Echo-Hawk’s friends and relatives — all under 55 — have died of covid.
“This is trauma. This is generational impact that we must have an intentional focus on. The scars are there,” said Marcella Nunez-Smith, chair of President Biden’s COVID-19 Health Equity Task Force and associate dean for health equity research at Yale University. “We can’t think that we’re going to test and vaccinate our way out of this deep pain and hurt.”
The pandemic has brought into stark relief centuries of entwining social, environmental, economic and political factors that erode the health and shorten the lives of people of color, putting them at higher risk of the chronic conditions that leave immune systems vulnerable to the coronavirus. Many of those same factors fuel the misinformation, mistrust and fear that leave too many unprotected.
Take the suggestion that people talk to their doctor about which symptoms warrant testing or a trip to the hospital as well as the safety of vaccines. Seems simple. It’s not.
Many people don’t have a physician they see regularly due in part to significant provider shortages in communities of color. If they do have a doctor, it can cost too much money for a visit even if insured. There are language barriers for those who don’t speak English fluently and fear of deportation among undocumented immigrants.
“Some of the issues at hand are structural issues, things that are built into the fabric of society,” said Enrique W. Neblett Jr., a University of Michigan professor who studies racism and health.
Essential workers who cannot avoid the virus in their jobs because they do not have the luxury of working from home. People living in multigenerational homes with several adult wage-earners, sharing housing because their pay is so low. Even the fight to be counted among the covid casualties — some states and hospitals, Echo-Hawk said, don’t have “even a box to check to say you are American Indian or Alaskan Native.”
It can be difficult to tackle the structural issues influencing the unequal burden of the pandemic while dealing with the day-to-day stress and worry it ignites, which, Neblett said, is why attention must focus on both long-term solutions and “what do we do now? It’s not just that simple as, ‘Oh, you just put on your mask, and we’ll all be good.’ It’s more complicated than that.”
The exacting toll of the last year and a half — covid’s stranglehold on communities of color and George Floyd’s murder — forced the country to interrogate the genealogy of American racism and its effect on health and well-being.
“This is an instance where we finally named it and talked about structural racism as a contributing factor in ways that we haven’t with other health disorders,” Neblett said.
But the nation’s attention span can be short. Polls show there was a sharp rise in concern about discrimination against Black Americans by police following Floyd’s murder, including among White Americans. That concern has eroded some since 2020, though it does remain higher than years past.
“This mistaken understanding that people have, almost this sort of impatience like, ‘Oh, we see racism. Let’s just fix that,’ that’s the thing that gives me hives,” Nunez-Smith said. “This is about generational investments and fundamental changes in ways of being. We didn’t get here overnight.”
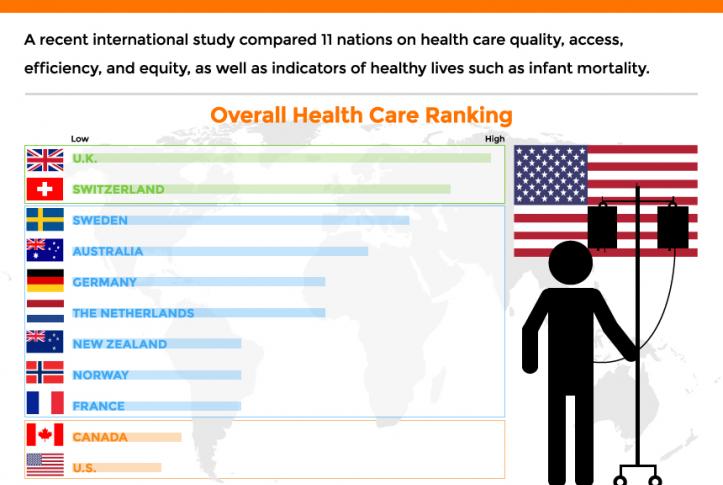
The performance of the U.S. healthcare system ranked last among 11 high-income countries, according to a report released Aug. 4 by the Commonwealth Fund.
To compare the performance of the healthcare systems in 11 high-income countries, the Commonwealth Fund analyzed 71 performance measures across five domains: access to care, care process, administrative efficiency, equity and patient outcomes.
Despite spending far more of its gross domestic product on healthcare than the other nations included in the report, the U.S. ranked last overall, as well as last for access to care, administrative efficiency, equity and patient outcomes. However, the U.S. ranked second on measures of care process, trailing only New Zealand.
Norway, the Netherlands and Australia had the best healthcare system performance, according to the report. In all seven iterations of the study conducted by the Commonwealth Fund since 2004, the U.S. has ranked last. It is the only country included in the study that does not provide its citizens with universal health insurance coverage.
Four features separate the top performing countries from the U.S., according to the report: universal health insurance coverage and removal of cost barriers; investment in primary care systems to ensure equitable healthcare access; reduction of administrative burdens that divert time and spending from health improvement efforts; and investment in social services, particularly for children and working-age adults.