We’ve closely tracked Colorado’s pursuit of its own public option insurance plan, which seems now to have reached a compromise that will allow a bill to move forward, according to reporting from Colorado Public Radio. The saga began two years ago when state legislators passed a law requiring Democratic Governor Jared Polis’ administration to develop a public option proposal. Amid the pandemic and broad industry opposition, progress stalled last year on the proposal. Lawmakers picked up the proposal this session, and have made progress on a compromise bill now poised to pass the state’s Democratic legislature.
Unlike the earlier version, the new legislation would not lay the groundwork for a government-run insurance option, but rather would force insurers to offer a plan in which the benefits and premiums are defined and regulated by the state. The bill would also allow the state to regulate how much hospitals and doctors are paid.
In the current version,hospital reimbursement is set at a minimum of 155 percent of Medicare rates, and premiums are expected to be 18 percent lower than the current average. While state Republicans and some progressive Democrats are still opposed, the Colorado Hospital Association and State Association of Health Plans are neutral on the bill, largely eliminating industry opposition.
The role hospitals played in fighting the pandemic surely paved the way toward the compromise bill, which is viewed as much more friendly to providers than the previous proposal.With the Biden administration unlikely to pursue Medicare expansion or a national public option, we expect more Democratic-run states to pursue these sorts of state-level efforts to expand coverage.
In the wake of the pandemic, providers are well-positioned to negotiate—and should use the goodwill they’ve generated to explore more favorable terms, rather than resorting to their usual knee-jerk opposition to these kinds of proposals.
The Centers for Medicare & Medicaid Services (CMS) released its 2022 Inpatient Prospective Payment System (IPPS) proposed rule this week. Overall, the rule brings good news for hospitals: Medicare reimbursement rates are slated to increase by 2.8 percent,resulting in a $2.5B payment boost to the industry.
In another win, hospitals will no longer be required to disclose their contract terms with Medicare Advantage (MA) insurers. Hospitals had previously been mandated by the 2021 rule to report median, payer-specific, negotiated charges for MA insurers on their Medicare cost reports. Medicare’s goal was to use this data to create a new, market-based, inpatient reimbursement methodology—an effort which has also been tabled, at least for now.
Led by the American Hospital Association, hospitals have been embroiled in lengthy legal challenges over a variety of CMS price transparency requirements, maintaining they are neither beneficial for consumers, nor helpful in lowering healthcare costs.
It’s too early to tell whether this step back from price transparency, which was a key goal of the Trump administration, signals anything about the Biden administration’s priorities; it’s possible CMS may just be slowing down the effort in the wake of the pandemic.
Other highlights of the proposed rule includefunding 1,000 more residency slots over the next five years, and extending payments for COVID-19 treatments to the end of 2022, as CMS expects COVID patients will need care beyond the duration of public health emergency. The agency also proposed several changes to its readmissions and other value-based purchasing programs, to ensure hospitals aren’t penalized by COVID-related impacts on quality measures.
Comments on the proposed rule are due by June 28th.
In his first address to a joint session of Congress, delivered on the eve of his 100th day in office, President Biden laid out his vision for two major legislative proposals to follow the $1.9T stimulus package he signed into law last month.
The first, described as an “infrastructure” bill, focuses largely on investing in transportation-related improvements, building projects, and “green” upgrades to the nation’s energy grid, along with a $400B investment in home-based care for the elderly and people with disabilities—which amounts to over 17 percent of the package’s $2.3T price tag.
The second, which he unveiled in Wednesday’s speech, is a $1.8T “families” bill, is largely aimed at expanding childcare subsidies, early childhood education, paid family and medical leave, and educational investments. Included in that package is $200B to extend the temporary subsidies—approved as part of last month’s stimulus law—for those seeking health insurance coverage on the individual marketplaces created by the Affordable Care Act (ACA).
Notably absent from either proposal were two categories of healthcare reform that received much focus and airtime during last year’s election campaign: reducing the cost of prescription drugs and lowering the eligibility age for Medicare to 60 or below. Given the closely divided makeup of the new Congress, and the relatively moderate position staked out by the Biden administration on healthcare issues (with a bias toward bolstering the ACA rather than pursuing sweeping changes), we’re not surprised to see the Medicare expansion go unmentioned.
But the bipartisan popularity of lowering prescription drug costs seems like a missed opportunity for Biden, who encouraged the Congress to return to it separately, later in the year. We’ll see. For now, with even some Democrats expressing concern about the $4.1T price tag of Biden’s proposals, we would be surprised if all $600B of the healthcare-related spending makes it to the final legislation. In particular, our guess is that some portion of the home-care spending will get traded away in favor of other components of the package. Expect negotiations to be intense.
Europe seems poised to set the global standard for vaccine passports, now that European Commission President Ursula von der Leyen has signaled that vaccinated Americans will be allowed to travel to the continent this summer.
Why it matters: Opening up travel to vaccinated Americans will bring new urgency to creating some kind of trusted means for people to prove they’ve been vaccinated, Axios’ Felix Salmon reports.
The big picture: There will probably never be a single credential that most people use to prove they’ve been vaccinated, for every purpose.
But the EU’s system will help set a standard for a proof of vaccination that’s both easily accessible and difficult to forge.
The U.S. is being closely consulted on the European passport, so any future American system will likely use similar protocols.
Details: Informal mechanisms like simply asking someone whether they’re had a shot can suffice in many situations. A system for international travel will likely be far more stringent. And there’s a wide middle, too.
Other activities that don’t need the same rigorous standards as international travel could rely on the CDC’s vaccination cards; options like a printed QR code, similar to what’s been proposed by PathCheck; or a digital QR code, like the ones created by CommonPass or the Vaccine Credential Initiative.
The bottom line:The world of vaccine passports is almost certainly going to end up as a mishmash of different credentials for different activities, rather than a single credential used by everybody for everything.
A new study out this week revived an old argument about whether telehealth visits spur more downstream care utilization compared to in-person visits, potentially raising the total cost of care. Researchers evaluated three years of claims data from Blue Cross Blue Shield of Michigan to compare patients treated for an acute upper respiratory infection via telemedicine versus an in-person visit, finding that patients who used telemedicine were almost twice as likely to have a related downstream visit (10.3 percent vs. 5.9 percent, respectively).
They concluded that these increased rates of follow-up likely negate any cost savings from replacing an in-person encounter with a less costly telemedicine visit.
Our take: so what?The study failed to address the question of whether a telemedicine visit was easier to access, or more timely than an in-person visit. Further, it evaluated data from 2016-2019, so the results should be caveated as pertaining to the “pre-COVID era”, before last year’s explosion in virtual care. Moreover, it’s unsurprising that patients who have a telemedicine visit may need more follow-up care (or that providers who deliver care virtually may be more aggressive about suggesting follow-up if symptoms change).
This focus on increased downstream care as a prima facie failure also ignores the fact that telemedicine services likely tap into pent-up, unmet demand for access to care. More access is a good thing for patients—and policymakers should consider that limiting reimbursement for virtual access to primary care (which accounts for less than 6 percent of total health spending) is unlikely to deliver the system-wide reduction in healthcare spending we need.
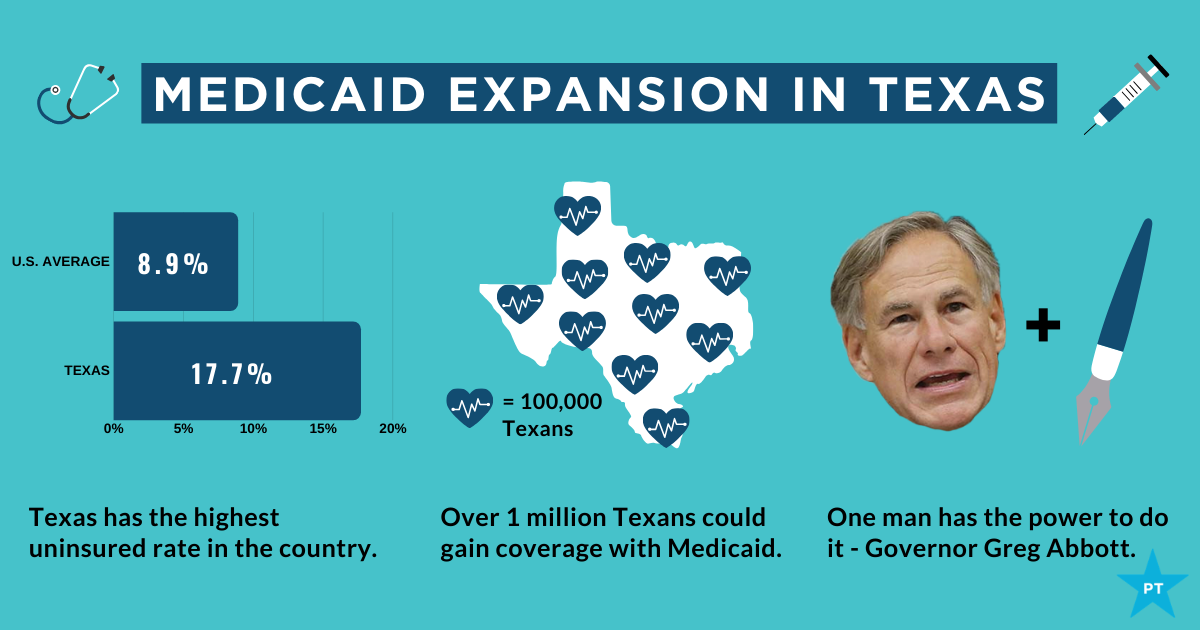
The showdown between the Biden administration and the state of Texas over Medicaid expansion continued to escalate this week. Sen. John Cornyn (R-TX) said he planned to place a hold on the confirmation of Chiquita Brooks-LaSure to become Administrator of the Centers for Medicare & Medicaid Services (CMS), until his concerns over the agency’s move last week to rescind a waiver extension previously granted by the Trump administration were addressed.
The so-called “1115 waiver”—worth more than $11B annually—would have extended by a decade Texas’ ability to use Medicaid funds to cover hospital costs for uninsured residents, rather than expanding Medicaid coverage under the Affordable Care Act (ACA). In rescinding the waiver extension, the Biden administration cited the lack of a public notice process before the waiver was granted, and said that the state’s existing waiver would instead expire next year, as previously scheduled.
Sources inside the administration told the Washington Post last week thatthe move was intended to force Texas’ hand on Medicaid expansion; the state is one of 12 that have not expanded Medicaid, leaving it with the largest share of uninsured residents of any state, with eligibility currently limited to pregnant women, children, people with disabilities, and families with monthly incomes under $300 per month, or 13.6 percent of the federal poverty level.
Enticing the dozen remaining holdout states to expand Medicaid is an important policy priority for the new administration.A key component of the recently passed American Rescue Plan Act is a package of enhanced incentives for those states to expand eligibility, offering an extended 90 percent federal match, in addition to increased funding for existing Medicaid populations.
Although none of the non-expansion states have budged yet, there has been renewed focus among state lawmakers on Medicaid expansion, including in Texas, where the idea had garnered bipartisan support. However, on Thursday, the Texas legislature voted down a proposal aimed at pushing the state toward expanding coverage for the uninsured, by an 80-68 margin. Meanwhile, the rescission of Texas’ waiver has angered the state’s Republican leadership, along with the Texas Hospital Association, whose members have benefited from the waiver’s use of funds to reimburse them for delivering uncompensated care.
While Cornyn’s hold will not ultimately stop the confirmation of the new CMS leader, the escalation on both sides over the past several days surely makes finding a compromise solution less likely. The Biden health policy team is said to be developing a new proposal, as part of an upcoming legislative package, to use the ACA marketplace to offer coverage to people in non-expansion states who might otherwise be eligible for Medicaid—yet another attempt to address one of the longest-standing points of contention stemming from the 2010 health reform law.
Of 26 health systems surveyed by MedCity News, nearly half used automated tools to respond to the Covid-19 pandemic, but none of them were regulated. Even as some hospitals continued using these algorithms, experts cautioned against their use in high-stakes decisions.
A year ago, Michigan Medicine faced a dire situation. In March of 2020, the health system predicted it would have three times as many patients as its 1,000-bed capacity — and that was the best-case scenario. Hospital leadership prepared for this grim prediction by opening a field hospital in a nearby indoor track facility, where patients could go if they were stable, but still needed hospital care. But they faced another predicament: How would they decide who to send there?
Two weeks before the field hospital was set to open, Michigan Medicine decided to use a risk model developed by Epic Systems to flag patients at risk of deterioration. Patients were given a score of 0 to 100, intended to help care teams determine if they might need an ICU bed in the near future. Although the model wasn’t developed specifically for Covid-19 patients, it was the best option available at the time, said Dr. Karandeep Singh, an assistant professor of learning health sciences at the University of Michigan and chair of Michigan Medicine’s clinical intelligence committee. But there was no peer-reviewed research to show how well it actually worked.
Researchers tested it on over 300 Covid-19 patients between March and May. They were looking for scores that would indicate when patients would need to go to the ICU, and if there was a point where patients almost certainly wouldn’t need intensive care.
“We did find a threshold where if you remained below that threshold, 90% of patients wouldn’t need to go to the ICU,” Singh said. “Is that enough to make a decision on? We didn’t think so.”
But if the number of patients were to far exceed the health system’s capacity, it would be helpful to have some way to assist with those decisions.
“It was something that we definitely thought about implementing if that day were to come,” he said in a February interview.
Thankfully, that day never came.
The survey Michigan Medicine is one of 80 hospitals contacted by MedCity News between January and April in a survey of decision-support systems implemented during the pandemic. Of the 26 respondents, 12 used machine learning tools or automated decision systems as part of their pandemic response. Larger hospitals and academic medical centers used them more frequently.
Faced with scarcities in testing, masks, hospital beds and vaccines, several of the hospitals turned to models as they prepared for difficult decisions. The deterioration index created by Epic was one of the most widely implemented — more than 100 hospitals are currently using it — but in many cases, hospitals also formulated their own algorithms.
They built models to predict which patients were most likely to test positive when shortages of swabs and reagents backlogged tests early in the pandemic. Others developed risk-scoring tools to help determine who should be contacted first for monoclonal antibody treatment, or which Covid patients should be enrolled in at-home monitoring programs.
MedCity News also interviewed hospitals on their processes for evaluating software tools to ensure they are accurate and unbiased. Currently, the FDA does not require some clinical decision-support systems to be cleared as medical devices, leaving the developers of these tools and the hospitals that implement them responsible for vetting them.
Among the hospitals that published efficacy data, some of the models were only evaluated through retrospective studies. This can pose a challenge in figuring out how clinicians actually use them in practice, and how well they work in real time. And while some of the hospitals tested whether the models were accurate across different groups of patients — such as people of a certain race, gender or location — this practice wasn’t universal.
As more companies spin up these models, researchers cautioned that they need to be designed and implemented carefully, to ensure they don’t yield biased results.
An ongoing review of more than 200 Covid-19 risk-prediction models found that the majority had a high risk of bias, meaning the data they were trained on might not represent the real world.
“It’s that very careful and non-trivial process of defining exactly what we want the algorithm to be doing,” said Ziad Obermeyer, an associate professor of health policy and management at UC Berkeley who studies machine learning in healthcare. “I think an optimistic view is that the pandemic functions as a wakeup call for us to be a lot more careful in all of the ways we’ve talked about with how we build algorithms, how we evaluate them, and what we want them to do.”
Algorithms can’t be a proxy for tough decisions Concerns about bias are not new to healthcare. In a paper published two years ago, Obermeyer found a tool used by several hospitals to prioritize high-risk patients for additional care resources was biased against Black patients. By equating patients’ health needs with the cost of care, the developers built an algorithm that yielded discriminatory results.
More recently, a rule-based system developed by Stanford Medicine to determine who would get the Covid-19 vaccine first ended up prioritizing administrators and doctors who were seeing patients remotely, leaving out most of its 1,300 residents who had been working on the front lines. After an uproar, the university attributed the errors to a “complex algorithm,” though there was no machine learning involved.
Both examples highlight the importance of thinking through what exactly a model is designed to do — and not using them as a proxy to avoid the hard questions.
“The Stanford thing was another example of, we wanted the algorithm to do A, but we told it to do B. I think many health systems are doing something similar,” Obermeyer said. “You want to give the vaccine first to people who need it the most — how do we measure that?”
The urgency that the pandemic created was a complicating factor. With little information and few proven systems to work with in the beginning, health systems began throwing ideas at the wall to see what works. One expert questioned whether people might be abdicating some responsibility to these tools.
“Hard decisions are being made at hospitals all the time, especially in this space, but I’m worried about algorithms being the idea of where the responsibility gets shifted,” said Varoon Mathur, a technology fellow at NYU’s AI Now Institute, in a Zoom interview. “Tough decisions are going to be made, I don’t think there are any doubts about that. But what are those tough decisions? We don’t actually name what constraints we’re hitting up against.”
The wild, wild west There currently is no gold standard for how hospitals should implement machine learning tools, and little regulatory oversight for models designed to support physicians’ decisions, resulting in an environment that Mathur described as the “wild, wild west.”
How these systems were used varied significantly from hospital to hospital.
Early in the pandemic, Cleveland Clinic used a model to predict which patients were most likely to test positive for the virus as tests were limited. Researchers developed it using health record data from more than 11,000 patients in Ohio and Florida, including 818 who tested positive for Covid-19. Later, they created a similar risk calculator to determine which patients were most likely to be hospitalized for Covid-19, which was used to prioritize which patients would be contacted daily as part of an at-home monitoring program.
Initially, anyone who tested positive for Covid-19 could enroll in this program, but as cases began to tick up, “you could see how quickly the nurses and care managers who were running this program were overwhelmed,” said Dr. Lara Jehi, Chief Research Information Officer at Cleveland Clinic. “When you had thousands of patients who tested positive, how could you contact all of them?”
While the tool included dozens of factors, such as a patient’s age, sex, BMI, zip code, and whether they smoked or got their flu shot, it’s also worth noting that demographic information significantly changed the results. For example, a patient’s race “far outweighs” any medical comorbidity when used by the tool to estimate hospitalization risk, according to a paper published in Plos One. Cleveland Clinic recently made the model available to other health systems.
Others, like Stanford Health Care and 731-bed Santa Clara County Medical Center, started using Epic’s clinical deterioration index before developing their own Covid-specific risk models. At one point, Stanford developed its own risk-scoring tool, which was built using past data from other patients who had similar respiratory diseases, such as the flu, pneumonia, or acute respiratory distress syndrome. It was designed to predict which patients would need ventilation within two days, and someone’s risk of dying from the disease at the time of admission.
Stanford tested the model to see how it worked on retrospective data from 159 patients that were hospitalized with Covid-19, and cross-validated it with Salt Lake City-based Intermountain Healthcare, a process that took several months. Although this gave some additional assurance — Salt Lake City and Palo Alto have very different populations, smoking rates and demographics — it still wasn’t representative of some patient groups across the U.S.
“Ideally, what we would want to do is run the model specifically on different populations, like on African Americans or Hispanics and see how it performs to ensure it’s performing the same for different groups,” Tina Hernandez-Boussard, an associate professor of medicine, biomedical data science and surgery at Stanford, said in a February interview. “That’s something we’re actively seeking. Our numbers are still a little low to do that right now.”
Stanford planned to implement the model earlier this year, but ultimately tabled it as Covid-19 cases fell.
‘The target is moving so rapidly’ Although large medical centers were more likely to have implemented automated systems, there were a few notable holdouts. For example, UC San Francisco Health, Duke Health and Dignity Health all said they opted not to use risk-prediction models or other machine learning tools in their pandemic responses.
“It’s pretty wild out there and I’ll be honest with you — the dynamics are changing so rapidly,” said Dr. Erich Huang, chief officer for data quality at Duke Health and director of Duke Forge. “You might have a model that makes sense for the conditions of last month but do they make sense for the conditions of next month?”
That’s especially true as new variants spread across the U.S., and more adults are vaccinated, changing the nature and pace of the disease. But other, less obvious factors might also affect the data. For instance, Huang pointed to big differences in social mobility across the state of North Carolina, and whether people complied with local restrictions. Differing social and demographic factors across communities, such as where people work and whether they have health insurance, can also affect how a model performs.
“There are so many different axes of variability, I’d feel hard pressed to be comfortable using machine learning or AI at this point in time,” he said. “We need to be careful and understand the stakes of what we’re doing, especially in healthcare.”
Leadership at one of the largest public hospitals in the U.S., 600-bed LAC+USC Medical Center in Los Angeles, also steered away from using predictive models, even as it faced an alarming surge in cases over the winter months.
At most, the hospital used alerts to remind physicians to wear protective equipment when a patient has tested positive for Covid-19.
“My impression is that the industry is not anywhere near ready to deploy fully automated stuff just because of the risks involved,” said Dr. Phillip Gruber, LAC+USC’s chief medical information officer. “Our institution and a lot of institutions in our region are still focused on core competencies. We have to be good stewards of taxpayer dollars.”
When the data itself is biased Developers have to contend with the fact that any model developed in healthcare will be biased, because the data itself is biased; how people access and interact with health systems in the U.S. is fundamentally unequal.
How that information is recorded in electronic health record systems (EHR) can also be a source of bias, NYU’s Mathur said. People don’t always self-report their race or ethnicity in a way that fits neatly within the parameters of an EHR. Not everyone trusts health systems, and many people struggle to even access care in the first place.
“Demographic variables are not going to be sharply nuanced. Even if they are… in my opinion, they’re not clean enough or good enough to be nuanced into a model,” Mathur said.
The information hospitals have had to work with during the pandemic is particularly messy. Differences in testing access and missing demographic data also affect how resources are distributed and other responses to the pandemic.
“It’s very striking because everything we know about the pandemic is viewed through the lens of number of cases or number of deaths,” UC Berkeley’s Obermeyer said. “But all of that depends on access to testing.”
At the hospital level, internal data wouldn’t be enough to truly follow whether an algorithm to predict adverse events from Covid-19 was actually working. Developers would have to look at social security data on mortality, or whether the patient went to another hospital, to track down what happened.
“What about the people a physician sends home — if they die and don’t come back?” he said.
Researchers at Mount Sinai Health System tested a machine learning tool to predict critical events in Covid-19 patients — such as dialysis, intubation or ICU admission — to ensure it worked across different patient demographics. But they still ran into their own limitations, even though the New York-based hospital system serves a diverse group of patients.
They tested how the model performed across Mount Sinai’s different hospitals. In some cases, when the model wasn’t very robust, it yielded different results, said Benjamin Glicksberg, an assistant professor of genetics and genomic sciences at Mount Sinai and a member of its Hasso Plattner Institute for Digital Health.
They also tested how it worked in different subgroups of patients to ensure it didn’t perform disproportionately better for patients from one demographic.
“If there’s a bias in the data going in, there’s almost certainly going to be a bias in the data coming out of it,” he said in a Zoom interview. “Unfortunately, I think it’s going to be a matter of having more information that can approximate these external factors that may drive these discrepancies. A lot of that is social determinants of health, which are not captured well in the EHR. That’s going to be critical for how we assess model fairness.”
Even after checking for whether a model yields fair and accurate results, the work isn’t done yet. Hospitals must continue to validate continuously to ensure they’re still working as intended — especially in a situation as fast-moving as a pandemic.
A bigger role for regulators All of this is stirring up a broader discussion about how much of a role regulators should have in how decision-support systems are implemented.
Of the hospitals surveyed by MedCity News, none of the models they developed had been cleared by the FDA, and most of the external tools they implemented also hadn’t gone through any regulatory review.
“My experience suggests that most models are put into practice with very little evidence of their effects on outcomes because they are presumed to work, or at least to be more efficient than other decision-making processes,” Kellie Owens, a researcher for Data & Society, a nonprofit that studies the social implications of technology, wrote in an email. “I think we still need to develop better ways to conduct algorithmic risk assessments in medicine. I’d like to see the FDA take a much larger role in regulating AI and machine learning models before their implementation.”
Developers should also ask themselves if the communities they’re serving have a say in how the system is built, or whether it is needed in the first place. The majority of hospitals surveyed did not share with patients if a model was used in their care or involve patients in the development process.
In some cases, the best option might be the simplest one: don’t build.
In the meantime, hospitals are left to sift through existing published data, preprints and vendor promises to decide on the best option. To date, Michigan Medicine’s paper is still the only one that has been published on Epic’s Deterioration Index.
Care teams there used Epic’s score as a support tool for its rapid response teams to check in on patients. But the health system was also looking at other options.
“The short game was that we had to go with the score we had,” Singh said. “The longer game was, Epic’s deterioration index is proprietary. That raises questions about what is in it.”
For some time, we’ve been focused on the efforts of Walmart to launch and grow a care delivery business, especially as it has piloted an expanded primary care clinic offering in a handful of states. We’ve long thought that access to basic care at the scale that Walmart brings could be transformative, given that more than half of Americans visit a Walmart store every week. Along those same lines, we’ve always wondered why Dollar General and Dollar Tree—each with around four times as many retail locations as Walmart—haven’t gotten into the retail clinic or pharmacy businesses.
(Part of the answer is ultra-lean staffing—this piece gives a good sense of the basic, and troubling, economics of dollar stores.) Now, as the federal government ramps up its efforts to widely distribute the COVID vaccines, it turns out that the CDC is actively discussing a partnership with Dollar General to administer the shots.
A fascinating new paper (still in preprint) from researchers at Yale shows why this could be a true gamechanger. The Biden administration, through its partnership with national and independent pharmacy providers, aims to have a vaccination site within five miles of 90 percent of the US population by next week. Compared to those pharmacy partners, researchers found,Dollar General stores are disproportionately located in areas of high “social vulnerability”, with lower income residents and high concentrations of disadvantaged groups. Particularly in the Southeast, a partnership with Dollar General would vastly increase access for low-income Black and Latino residents, allowing vaccine access within one mile for many, many more people. And the partnership could form the basis for future expansions of basic healthcare services to vulnerable and rural communities, particularly if some of the $7.5B in funding for COVID vaccine distribution went to helping dollar store locations bolster staffing and equipment to deliver basic health services. We’ll be watching with interest to see if the potential Dollar General partnership comes to fruition.
As health systems look to address the “social determinants of health”, one obvious but often overlooked place to start is with their own employees. The left side of the graphic below shows forecasted employment growth and salaries across a range of healthcare occupations. Many of the fastest-growing healthcare jobs—including home health and personal aides, medical assistants, and phlebotomists—are among the lowest-paid.
Case in point: home health and personal care aides are among the top 20 fastest-growing occupations in the US, and median wage for these jobs is only about $12 per hour, or around 200 percent of the federal poverty level—well below the living wage in many parts of the nation. (Note that this analysis does not include support staff who are not healthcare specific, like custodial or dietary workers, so the number of low-wage workers at health systems is likely higher.)
Among of the many struggles lower-income healthcare employees face is finding affordable housing. Using fair market rent data from the US Department of Housing and Urban Development, the right side of the graphic shows that healthcare support workers, even at the 90th percentile salary level, struggle to afford rent in the majority of the 50 largest US metros areas. In particular, home health aides in the top decile of earners can only afford rent in 14 percent of major cities.
These disparities have caught the attention of lawmakers. The $400B in President Biden’s proposed infrastructure plan devoted to home healthcare for seniors includes tactics to increase the wages and quality of life for these caregivers. But as we await policy solutions, health systems should pay careful attention to issues of housing insecurity and other structural challenges facing their workers and look to increase wages and provide targeted support to these critical team members.