https://www.healthcaredive.com/news/we-feel-bullish-payers-look-ahead-to-2021/585211/

Top executives at some of the biggest commercial insurers outlined their shifting strategies and what markets are growth opportunities in light of the recession at Morgan Stanley’s annual conference.
Top executives at some of the biggest commercial insurers provided a peak behind their curtains at Morgan Stanley’s annual investor conference this week, discussing the pace of utilization recovery and how they’re approaching rate setting and risk going into next year
Though there’s significant uncertainty around the future of the insurance industry, many remarks can be summed up in a line from Cigna CEO David Cordani: “We feel bullish on 2021.”
And despite the major role of government in regulating healthcare, most officials seemed agnostic on the presidential election looming in less than two months.
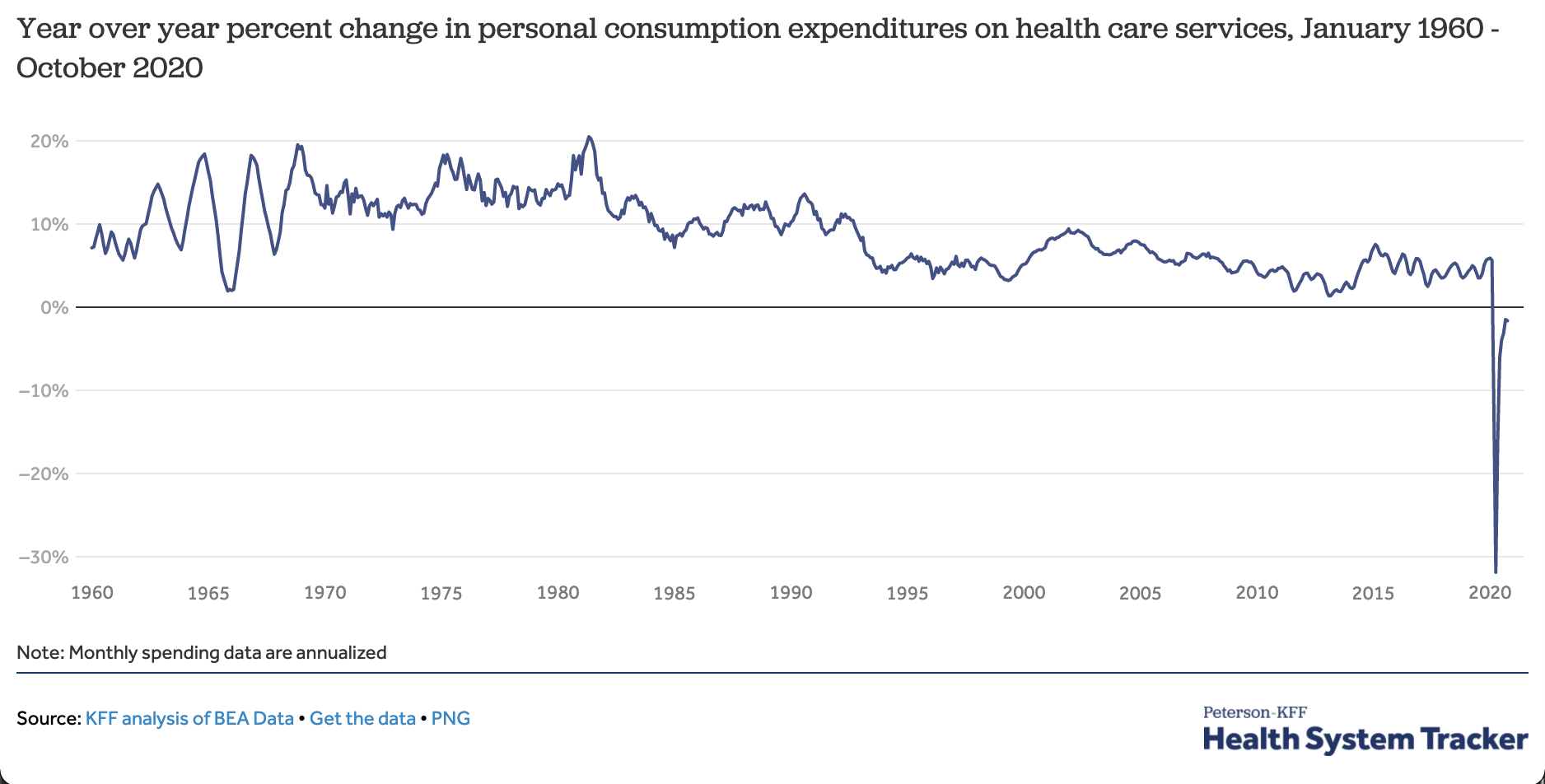
Payers are reporting skyrocketing profits amid the COVID-19 pandemic as patients deferred care in droves in the second quarter, sparking a congressional investigation into business practices. Use of healthcare services continues to recover from a nadir in March and April, and that recovery has continued into the third quarter, payer executives said. But the pace has differed by segment.
At the start of the pandemic, Humana saw beneficiary use drop to about 30% of pre-COVID-19 levels until mid-May, when it slowly started to tick back up. The Louisville, Kentucky-based insurer’s utilization is now still “a little below par,” but well above that depression and meeting internal expectations, CEO Bruce Broussard said.
CVS Health-owned Aetna has seen its commercial business come back faster than Medicare, CFO Eva Boratto said. Primary care and labs have seen a quicker rebound, but it’s been slower in inpatient and ambulatory.
Centene CEO Michael Neidorff predicts utilization will be between 65% to 80% of normal by the end of the year, but remains cautious due to the shifting nature of the pandemic, and how it could coincide with a potentially nasty flu season.
“We don’t know what other peaks we’re going to see,” Neidorff said.
2021 rate setting, strategic pivots
Unsurprisingly, COVID-19 is also shaping major payer’s go-to-market approaches and how they’re thinking about 2021 bids.
Humana, for example, studied both historical data prior to COVID-19 and did scenario planning around what the pandemic could do to factors like utilization, testing and treatment if it continued throughout the year. Eventually, the payer decided to base bid assumptions off trending historical information forward, according to Broussard.
“We were very oriented to pricing that was more conservative as we thought about the approach,” he said.
It appears Centene, contrastingly, is using 2020 data to risk score. When asked how the payer is approaching rate setting, Neidorff said: “We’re dealing with this year. And we’re saying that any concessions this year should not necessarily carry into next year, which is an entirely different year.”
Employers and plans nationwide are struggling with this issue. Only about 60% of employers are using 2020 claims to set rates for next year, while another 26% are calculating expected medical costs based on data from 2019, and 9% are using data from the first two months of 2020 alone, according to Credit Suisse.
The pandemic has also shifted insurers’ broader strategic priorities in 2021 and beyond, especially by hammering home the need for diversified revenue streams to keep afloat, top execs said.
“We’re in 37 states. If you have a stock that’s not performing well in your portfolio, you probably have some that are offsetting it,” Centene’s Neidorff said.
Humana has been investing in telesales, at-home and in-community offerings and digital capabilities, with an eye for growth. Broussard said Humana’s customers have been mostreactive to an omnichannel approach to care delivery.
For example, the payer is seeing home as an increasingly valid path for care a little more acute in service than in the past. As a result, Humana plans to continue investing in areas that dovetail with that trend, and those with biggest impact on downstream healthcare costs, including primary care, social determinants of health, behavioral health and pharmacy.
CVS has also accelerated development of its virtual care offering, eClinic, as a result of the pandemic and relaxed federal regulations. Visits are up 40% since the end of June, CEO Larry Merlo said, noting he believes the future of healthcare delivery is at the intersection between digital and physical.
Because of the pandemic, “we are seeing an accelerated shift to this multichannel, integrated approach,” Merlo said. “We did change some of our priorities, and accelerate some things that may have been further down the road.”
CVS is continuing to convert existing stores to health- and wellness-focused locations, called HealthHUBs, which devote a fifth of floor space to healthcare products and services. Currently, the Rhode Island-based giant has 275 HUBs up and running, despite pausing conversions for a time in March.
Cigna is also looking to drive revenue by moving beyond a payer’s traditional wheelhouse. On Wednesday, the insurer announced it was rebranding its health services division as Evernorth, in a next step for the Cigna-Express Scripts megamerger completed almost two years ago.
For its part, Centene is introducing more value-based contracts in 2021, after seeing providers it contracts with in alternative payment models are reporting stronger cash flow and patient relationships amid COVID-19 than those in fee-for-service relationships.
Going into next year, the payer is also focused on margin expansion, working with states to set rates and federal lobbying for friendly policies like an increased Medicaid match rate, Neidorff said.
Attractive markets
The COVID-19 recession booted millions of Americans off employer-sponsored insurance, though the full scope of the insurance crisis isn’t yet clear. Cigna’s Cordani noted the disenrollment in the first half of the year in its commercial population was lower than expected, helped by the fact the payer is less active in sectors hit hardest by the pandemic like travel and leisure.
But disenrollment could still snowball in the second half of 2020. As a result, a number of major commercial payers are building out offerings in two coverage backstops in the market: Medicaid and the Affordable Care Act exchanges.
Broussard said Humana sees ample opportunity in Medicaid — including the dually eligible — but wants to be more surgical in expansion moving forward, especially as states look for a more contemporary delivery of services and engagement with clinical programs. Humana is going to look for tuck-in acquisitions.
“Is there a way to enter the market in a small way, and leverage our capabilities and grow from that?,” Broussard said.
Cordani agreed that budget-strapped states are looking for new ways to lower costs, but said “Medicaid has always been a lower priority growth platform” for Cigna. Instead, the insurer sees the safety net program as an opportunity for Evernorth in the near term, more than its government business.
Of the 1.1 million new members Centene added from March through August, the majority were in Medicaid, but a significant portion were in the ACA exchanges, Neidorff said. Capitalizing on that momentum, Centene — already the largest payer in the exchanges — is adding 2 new states to its footprint for 2021. “I think we’ll grow in marketplace, given the level of people and the subsidies they get,” Neidorff said. “I see it as a positive going forward.”
Humana, however, is leery on entering the exchange market, given political uncertainty around the upcoming 2020 presidential election, according to its top exec.
“The exchange market has stabilized in a lot of different ways, but still has elements where it tends to be a sicker, more transient population,” Broussard said. “We’d rather not be in the situation where we go in and have to pull out because of the political realm.”
Payers also continue to forecast strong growth in Medicare Advantage. Currently, about 34% of Medicare beneficiaries are in the privately run Medicare plans. It’s a popular program: The Congressional Budget Office predicts MA’s share of the overall Medicare population will swell to 47% by 2029.
CVS is currently on track for mid-single-digit growth next year, and sees Aetna’s continued growth in MA as one of the building blocks to continued earnings power, Boratto said.
Similarly, Cigna is well on track to meeting its goal of 10% to 15% annual organic growth in MA, Cordani said. Historically, Cigna has only been present in about 18% to 19% of the addressable government market, but is trying to eventually expand to 50%.
Shrugging off election
Unlike years past when some payers worried of Democratic plans for Medicare and other aspects of insurance, most executives seemed to shrugged off the coming presidential election.
President Donald Trump has made undermining the ACA one of the chief goals of his first term, while Democrat nominee former Vice President Joe Biden’s healthcare plan revolves around shoring up the decade-old law, enacting a public option and lowering Medicare’s age of eligibility.
But executives noted Trump’s tenure hasn’t necessarily been bad for them, and having Biden at the helm could provide some opportunity for savvy operators.
Humana could be particularly at risk going into a period of political uncertainty. The payer has a smaller portfolio and fewer assets than some of its bigger peers, Ricky Goldwasser, managing director at Morgan Stanley, said.
But Broussard said regardless of whether the inhabitant of the White House is blue or red, they’ll likely support value-based payment models — a key tenet of its strategy. Additionally, the seemingly-threatening Medicare buy-in option is “very similar to MA,” Broussard said. “We’d see that as the opportunity to expand our ability to bring our capabilities to maybe a younger population, but with a lot of the same elements.”
Some industry experts see the public option, which has bipartisan support among voters, as a potential benefit for companies with leading market share in MA, like UnitedHealth, Humana and Aetna.
“We’ve had public options and done well in public options. So history says that’s fine,” Centene’s Neidorff said. “I think Biden would not be a threat, but an opportunity. I think a Trump re-election would just be more of what we’ve seen. And we’ve done OK with that.”