UnitedHealth Group, both the nation’s largest health insurer and largest employer of physicians, just announced plans to continue to rapidly grow the number of physicians in its Optum division.
This week CEO Dave Wichmann told investors in the company’s fourth quarter earnings call that Optum entered 2021 with over 50,000 employed or affiliated physicians, and expects to add at least 10,000 more across the year.(For context,HCA Healthcare, the largest for-profit US health system, employs or affiliates with roughly 46,000 physicians, and Kaiser Permanente employs about 23,300.) Optum is already making progress toward its ambitious goal with the announcement last week that the company is in talks to acquire Atrius Health, a 715-physician practice in the Boston area.
As was the case with other health plans, United’s health insurance business took an expected hit last quarter due to increased costs from COVID testing and treatment, combined with rebounding healthcare utilization. Optum, however, saw revenue up over 20 percent, which drove much of the company’s overall fourth quarter growth.
Expect United, and other large insurers, flush with record profits from last year, to continue to expand their portfolio of care, digital and analytics assets(see also Optum’s recently announced plan to acquire Change Healthcare for $13B) as they looks to grow integrated insurance and care delivery offerings.
It’s part of what we expect to be a 2021 “land grab” for strategic advantage in healthcare, as providers, health plans, and disruptors look to create comprehensive platforms to secure long-term consumer loyalty.
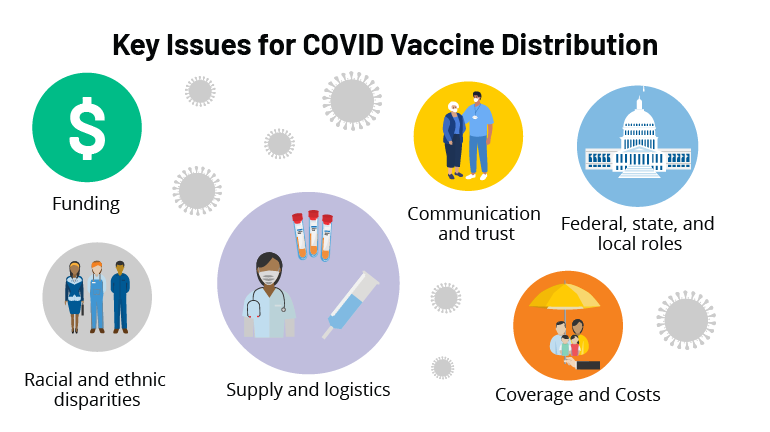
Although only 17 states are currently reporting data on the racial and ethnic breakdown of vaccine recipients, the early data indicate that there are significant disparities in who is getting vaccinated, with the share of Black and Latino people among vaccinees lower than their share of the total population in those states.
Alarmingly, in our recent conversations with health system executives,those same disparities seem to be present among healthcare workers employed by hospitals and health systems. Anecdotally, across a half-dozen health systems we’ve spoken with in the past week, most report that they’ve had about 70 percent of their workers agree to get the first dose of the COVID-19 vaccine.
However, that number looks significantly different when broken down by race and ethnicity:on average, the uptake rate among White, Asian, and Pacific Islander workers has been closer to 90-95 percent, while among Black and Latino workers, it’s been closer to 30-40 percent. Bear in mind these are employees of health systems—in many cases they’re frontline caregivers—and given their work environments you might expect them to be less hesitant to get the vaccine.
That 30-40 percent uptake rate is very worrisome, in two ways:caregivers outside of hospital settings, especially home care and nursing home workers, likely include a larger number of workers hesitant to get vaccinated. And in the general population, among whom health literacy is presumably much lower than among healthcare workers,it’s precisely those populations who are at highest risk of COVID infection, hospitalization, and death. (A further complication: health systems made it easy for their employees to get the shot. With vaccines for the general population still scarce, at-risk populations will inevitably have the most difficult time getting signed up, even if they want the vaccine.)
If health systems are the canary in the coal mine for vaccine hesitancy rates, we’re in for a tough challenge in getting the most vulnerable populations vaccinated in the months to come.
If you, like us, wanted to reach into your television this week, tap former President Bill Clinton on the shoulder and remind him to pull up his mask while attending the inauguration, a piece by New York Times science writer James Gorman says you weren’t alone, posing the question: “Is mask-slipping the new manspreading?”
Just as every man on a plane or bus does not “manspread” into the middle seat, not every man’s mask slips off his nose. But whether you’re watching the inauguration or milling around the grocery store, it does seem that men are far more likely than women to be found with their mask dangling at their chins. Gorman notes it’s unlikely that the shape of men’s noses or their need for more air flow account for the mask-slipping.
And, examples seem to abound across the political spectrum (see also Chief Justice John Roberts at the inauguration), so it’s not a Republican or Democratic thing.It’s a man thing. Also in this category: the dude on every airline flight we’ve taken in the past year, often outfitted in a Titleist cap and Greg Norman polo, who sports a neck gaiter plucked from his ski bag instead of a real mask (despite the large body of highly publicized evidence noting the gaiters’ inferior performance).
His demeanor says, “I am paying lip service to this mask rule, but I don’t like it. Now I will pull down my gaiter and slowly nurse this whiskey and soda until we land.” Perhaps men are less afraid of catching COVID, or, as some surveys suggest, ignoring mask rules is seen as a sign of machismo. But regardless of the motivation, fellas, we need you to wear your masks.And pull them up over your nose.
As vaccine eligibility guidelines have expanded to include adults over 65, we’ve heard from several friends and acquaintances looking for the inside scoop on getting a place in line. They’ve heard that their local health system is taking appointments, but only for established patients—do we know someone at the local system who could help them (or their mother, or their aunt with Stage IV cancer) get the shot?
One acquaintance was livid that his local hospital was prioritizing established patients:“They’re just rewarding people who have already paid them money. Is that fair?” It’s likely that system was making decisions based not on prior business relationships, but rather logistics. If patients are already “in the system”, they can be contacted and scheduled through the patient portal, fill out information online, and have their doses tracked in the EMR.
As health systems have been thrust into leading frontline vaccine distribution some have recognized an unprecedented opportunity to earn loyalty by connecting current and potential patients with the vaccine.
Outreach must provide clear information around vaccine access and how eligibility decisions are made(consider the difference in message between “we’re offering vaccines to current patients only”, and “because established patients can be quickly scheduled and monitored, we are beginning with this group, and plan to expand quickly”).
Systems’ ultimate goal should be getting vaccines to as many people as possible, as fast as possible, given supply and resource constraints.
As one of his first official actions upon taking office Wednesday, President Biden signed an executive order implementing a federal mask mandate, requiring masks to be worn by all federal employees and on all federal properties, as well as on all forms of interstate transportation. Yesterday Biden followed that action by officially naming his COVID response team, and issuing a detailed national plan for dealing with the pandemic. Describing the plan as a “full-scale wartime effort”, Biden highlighted the key components of the plan in an appearance with Dr. Anthony Fauci and COVID response coordinator Jeffrey Zients.
The plan instructs federal agencies to invoke the Defense Production Act to ensure adequate supplies of critical equipment, including masks, testing equipment, and vaccine-related supplies; calls for new nationalguidelines to help employers make workplaces safe for workers to return to their jobs, and to make schools safe for students to return; and promises to fully fund the states’ mobilization of the National Guard to assist in the vaccine rollout.
Also included in the plan is a new Pandemic Testing Board, charged with ramping up multiple forms of COVID testing; more investment in data gathering and reporting on the impact of the pandemic; and the establishment of a health equity task force, to ensure that vulnerable populations are an area of priority in pandemic response.
But Biden can only do so much by executive order. Funding for much of his ambitious COVID plan will require quick legislative action by Congress, meaning that the administration will either need to garner bipartisan support for its proposed “American Rescue Plan” legislation, or use the Senate’s budget reconciliation process to pass the bill with a simple majority (with Vice President Harris casting the tie-breaking vote). Even that may prove challenging, given skepticism among Republican (and some moderate Democratic) senators about the $1.9T price tag for the legislation.
We’d anticipate intense bargaining over the relief package—with broad agreement over the approximately $415B in spending on direct COVID response, but more haggling over the size of the economic stimulus component, including the promised $1,400 per person in direct financial assistance, expanded unemployment insurance, and raising the federal minimum wage to $15 per hour.
Some of the broader economic measures, along with the rest of Biden’s healthcare agenda and his larger proposals to invest in rebuilding critical infrastructure, may have to wait for future legislation, as the administration prioritizes COVID relief as its first—and most important—order of business.