Anthem has captured the attention of multiple hospitals and health systems across the U.S. as allegations of underpayment and inappropriate denials accumulate.
The insurer has been forced to pay millions already and continues to face off with providers.
Anthem is facing allegations of $70 million in unpaid claims from Portland-based MaineHealth. The health system said earlier this year that its flagship hospital, Maine Medical Center, would no longer contract with the insurer after its contract expires next year. Jeffrey Barkin, MD, president of the Maine Medical Association, said other providers in the state are leaving Anthem for the same reason.
In Georgia, the state insurance commissioner fined Anthem Blue Cross Blue Shield $5 million in March for failing to pay in a timely manner, delays in loading provider contracts and inaccurate provider directories.
VCU Health in Richmond, Va., said last year that 40 percent of its claims with Anthem were more than 90 days old and the insurer owed $385 million, according to the Richmond Times-Dispatch. The Virginia Hospital and Healthcare Association said Anthem has hundreds of millions of dollars in late and unpaid claims to hospitals across the state.
Eleven Indiana hospitals have also had trouble with Anthem. The hospitals alleged Anthem’s reimbursement system added a $50 triage fee and asked for additional patient records to avoid denial for 60 to 70 percent of thousands of emergency room claims from 2017-20. The hospitals alleged the strategy breached their contract with Anthem because hospitals are required to stabilize all patients requesting emergency services. A federal arbiter recently ordered Anthem to pay $4.5 million to the hospitals and said the insurer cannot use its list of diagnostic codes to downgrade or deny claims.
The Indiana hospitals are still counting the denied claims and said they are owed $12 million from Anthem due to downgraded claims.
The American Hospital Association accused Anthem of asking for prior authorizations for routine surgeries as roadblocks to patient care in a letter sent to the insurer last year.In 2021, 53 percent of Anthem’s medical bills for the second quarter were unpaid, amounting to $2.5 billion, according to the Times-Dispatch report.
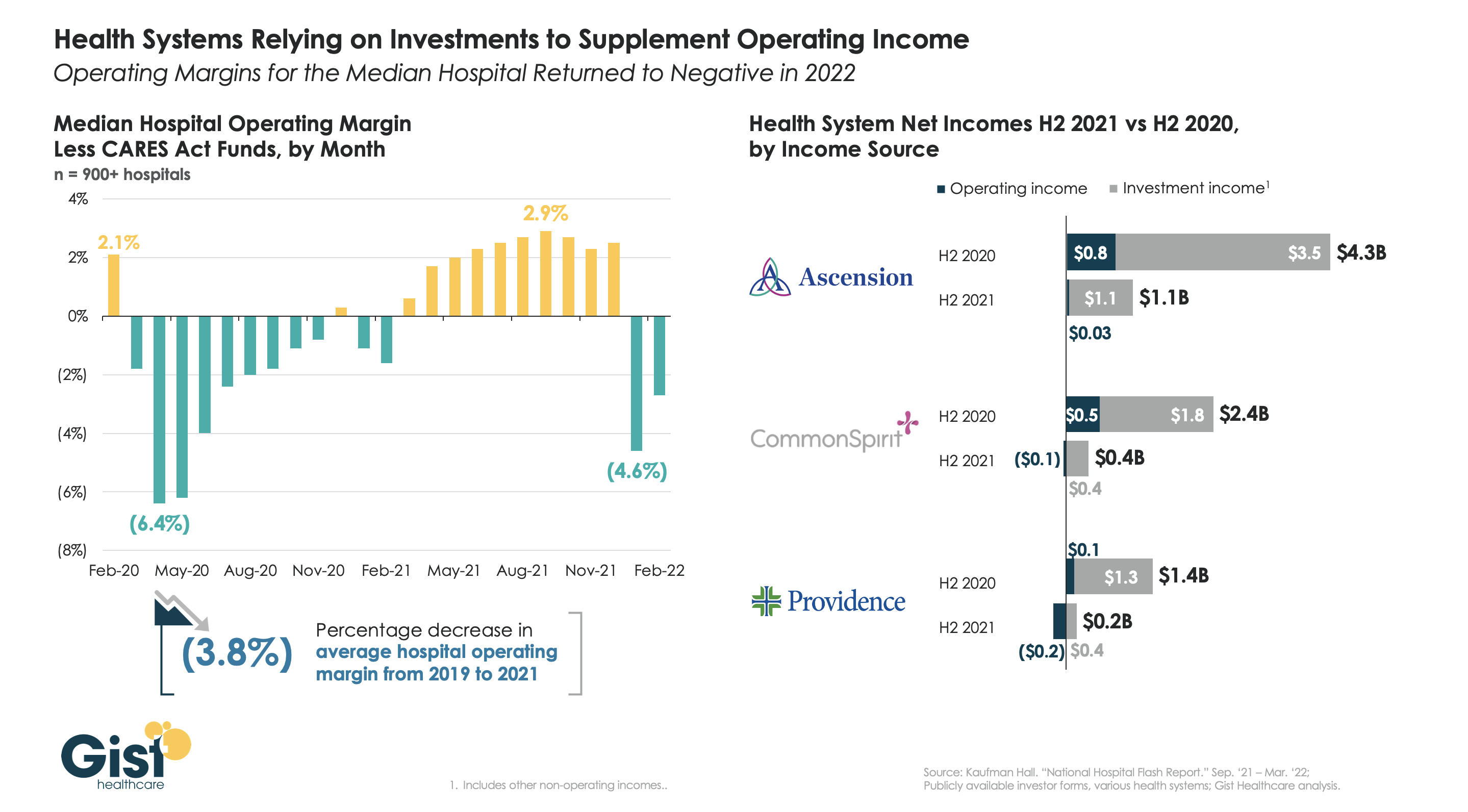
The combination of the Omicron surge, lackluster volume recovery, and rising expenses have contributed to a poor financial start of the year for most health systems. The graphic above shows that, after a healthier-than-expected 2021,the average hospital’s operating margin fell back into the red in early 2022, clocking in more than four percent lower than pre-pandemic levels.
Despite operational challenges, however, many of the largest health systems continue to garner headlines for their sizable profits, thanks to significant returns on their investment portfolios in 2021.
While CommonSpirit and Providence each posted negative operating margins for the second half of 2021, and Ascension managed a small operating profit, all three were able to use investment income to cushion their performance.
A growing number of health systems are doubling down on investment strategies in an effort to diversify revenue streams, and capture the kind of returns from investments generated by venture capital firms. However, it is unlikely that revenue diversification will be a sustainable long-term strategy.
To succeed, health systems must look to reconfigure elements of the legacy business model that are proving financially unsustainable amid rising expenses, shifts of care to lower-cost settings, and an evolving, consumer-centric landscape.
Salt Lake City-based Intermountain and Broomfield, CO-based SCL Health have now formed a 33-hospital, $14B nonprofit health system, which immediately becomes the 11th largest nationwide. The system will operate across seven states under the Intermountain brand, although the SCL hospitals will keep their legacy names and Catholic affiliation. Regulators signed off on the interstate merger after the systems agreed not to close any locations or services.
The Gist: Intermountain has been trying to build scale across the Mountain West in the last few years, having recently come up short in an attempt to merge with South Dakota-based Sanford Health.
The SCL deal will allowIntermountain to expand its SelectHealth insurance plan and integrated care model into the fast-growing Denver metro area, as well as into Kansas and Montana. As with any merger, the difficult work of combining cultures and demonstrating meaningful value for patients and consumers lies ahead.
While healthcare workers battle burnout, hospitals have been ramping up wages and other benefits to recruit and retain workers. It has created a culture of competition among health systems as well as travel agencies that offer considerably higher pay.
But other healthcare organizations are not hospitals’ only competitors. Some hospitals, particularly those in rural areas, are struggling to match rising employee pay among nonindustry employers such as Target and Walmart.
“We monitor and we’ve been looking and we ask around in the community and we can ask who’s paying what,” Troy Bruntz, CEO of Community Hospital in McCook, Neb., told Becker’s. “So we know where Walmart is on different things, and we’re OK. But if Walmart tried to match what Target’s doing, that would not be good.”
At Target, the hourly starting wage now ranges from $15-$24. The organization is making a $300 million investment total to boost wages and benefits, including health plans. Starting pay is dependent on the job, the market and local wage data, according to NPR.
Walmart raised the hourly wages for 565,000 workers in 2021 by at least $1 an hour, The New York Times reported. The company’s average hourly wage is $16.40, with the lowest being $12 and the highest being $17.
Meanwhile, Costco raised its minimum wage to $17 an hour, according to NPR. The federal minimum wage is $7.25.
Estimated employment for healthcare practitioners and technical occupations is 8.8 million, according to the latest data released March 31 by the U.S. Bureau of Labor Statistics. This includes nurse practitioners, physicians, registered nurses, physician assistants and respiratory therapists, among others.
In sales and related occupations, estimated employment is 13.3 million, according to the bureau. This includes retail salespersons, cashiers and first-line supervisors of retail salespersons, among others.
While retail companies up their wages, at least one hospital CEO is monitoring the issue. Healthcare leaders weigh their options
Mr. Bruntz said rising wages among retailers is an issue his organization monitors. Although Target does not have a store in McCook, there is a Walmart, where pay is increasing.
“I was quoted a few months ago saying Walmart was approaching $15 an hour, and we can handle that,” Mr. Bruntz said. “But when it gets to $20 or $25, it’s going to be an issue.”
He also said he cannot solely increase the wages of the people making less than $15 or less than $25 because he has to be fair in terms of wages for different types of roles.
Specifically, he said he is concerned about what matching rising wages at retailers would mean for labor expenses, which make up about half of the hospital’s cost structure.
“I double that half, that’s 25 percent more expenses instantly,” Mr. Bruntz said. “And how is that going to ratchet to a bottom line anything less than a massive negative number? So it’s a huge problem.”
Clinical positions are not the only ones hospitals and health systems are struggling to fill; they are encountering similar difficulties with technicians and food service workers. Regarding these roles, competition from industries outside healthcare is particularly challenging.
This is an issue Patrice Weiss, MD, executive vice president and chief medical officer of Roanoke, Va.-based Carilion Clinic, addressed during a Becker’spanel discussion April 4. The organization saw workforce issues not just in its clinical staff, but among environmental services staff.
“When you look at what … even fast food restaurants were offering to pay per hour, well gosh, those hours are a whole lot better,” she said during the panel discussion. “There’s no exposure. You’re not walking into a building where there’s an infectious disease or patients with pandemics are being admitted.”
Amid workforce challenges, Community Hospital is elevating its recruitment and retention efforts.
Mr. Bruntz touted the hospital as a hard place to leave because of the culture while acknowledging the monetary efforts his organization is making to keep staff.
He said the hospital has a retention program where full-time employees get a bonus amount if they are at the employer on Dec. 31 and have been there at least since April 15. Part-time workers are also eligible for a bonus, though a lesser amount.
“It also encourages staff [who work on an as-needed basis] to go part-time or full-time, and [those who are] part-time to go full-time,” Mr. Bruntz said. “That’s another thing we’re doing is higher amounts for higher status to encourage that trend.”
Additionally, Community Hospital, which has 330 employees, offers a referral bonus to staff to encourage people they know to come work with them.
“We want staff to bring people they like. [We are] encouraging staff to be their own ambassadors for filling positions,” Mr. Bruntz said.
He said the hospital also will offer employees a sizable market wage adjustment not because of competition from Walmart but because of inflation.
Graham County Hospital in Hill City, Kan., is also affected by the tight labor market, although it has not experienced much competition with retail companies, CEO Melissa Atkins told Becker’s. However, the hospital is struggling with competition from other healthcare organizations, particularly when it comes to patient care departments and nursing. While many hospitals have struggled to retain employees from travel agencies, Graham County Hospital has mostly been able to avoid it.
“As the demand increases, so does the wage,” Ms. Atkins said. “In addition to other hospitals offering sign-on bonuses and increased wages, nurse agency companies are offering higher wages for traveling nurse aides and nurses. We are extremely fortunate in that we have not had to use agency nurses. Our current staff has stepped up and filled in the shortages [with additional incentive pay].”
To combat this trend, the hospital has increased hourly wages and shift differentials, as many healthcare organizations have done. It has also provided bonuses using COVID-19 relief funds.
Overall, Mr. Bruntz said he prefers “not to get into an arms race with wages” among nonindustry competitors.
“It’s not going to end well for anybody. We prefer not to use that,” he said. “At the same time, we’re trying to do as much as possible without being in a full arms race. But if Walmart started paying $25 for a door greeter and cashier, we would have to reassess.”
UPDATE: April 14, 2022: Nurses will begin striking April 25 if they are unable to reach a deal with the system by then, according to a Wednesday statement from the union. The two sides have met with a federal mediator three times, and the strike would be open-ended.
Dive Brief:
Unionized nurses at Stanford hospitals in California voted in favor of authorizing a strike Thursday, meaning more than 4,500 nurses could walk off the job in a bid for better staffing, wages and mental health measures in new contracts.
Some 93% of nurses represented by the Committee for Recognition of Nursing Achievement voted in favor of the work stoppage, though the union did not set a date, according to a union release. It must give the hospitals 10 days notice before going on strike.
Nurses’ contracts expired March 31 and the union and hospital have engaged in more than 30 bargaining sessions over the past three months, including with a federal mediator, according to the union.
Dive Insight:
As the COVID-19 pandemic has worsened working conditions for nurses, some unions have made negotiating contracts a priority. Better staffing is key, along with higher wages and other benefits to help attract and retain employees amid ongoing shortages.
The California nurses’ demands in new contracts focus heavily on recruitment and retention of nursing staff “amid an industry-wide shortage and nurses being exhausted after working through the pandemic, many in short-staffed units,” the union said in the release.
They’re also asking for improved access to time off and more mental health support.
Nurses say their working conditions are becoming untenable and relying on travel staff and overtime shifts is not sustainable, according to the release.
The hospitals are taking precautionary steps to prepare for a potential strike and will resume negotiations with the union and a federal mediator Tuesday, according to a statement from Stanford.
But according to CRONA, nurses have filed significantly more assignment despite objections documents from 2020 to 2021 — forms that notify hospital supervisors of assignments nurses take despite personal objections around lacking resources, training or staff.
And a survey of CRONA nurses conducted in November 2021 founds that as many as 45% were considering quitting their jobs, according to the union.
That’s in line with other national surveys, including one from staffing firm Incredible Health released in March that found more than a third of nurses said they plan to leave their current jobs by the end of this year.
The CRONA nurses “readiness to strike demonstrates the urgency of the great professional and personal crisis they are facing and the solutions they are demanding from hospital executives,” the union said in the release.
No major strikes among healthcare workers have occurred so far this year, though several happened in 2021 and in 2020, the first year of the pandemic.
The formal end of the pandemic could swell the ranks of uninsured children by 6 million or more as temporary reforms to Medicaid are lifted.
Why it matters: Gaps in coverage could limit access to needed care and widen health disparities, by hitting lower-income families and children of color the hardest, experts say.
The big picture: A requirement that states keep Medicaid beneficiaries enrolled during the public health emergency in order to get more federal funding is credited with preventing a spike in uninsured adults and kids during the crisis.
Children are the biggest eligibility group in Medicaid, especially in the 12 states that haven’t expanded their Medicaid programs under the Affordable Care Act.
The lifting of the public health emergency, which was just extended to July 15, will lead states to determine whether their Medicaid enrollees are still eligible for coverage — a complicated process that could result in millions of Americans being removed from the program.
That would more than double the number of uninsured kids, which stood at 4.4 million in 2019.
“It is a stark, though we believe conservative, estimate,” said Joan Alker, the center’s executive director. “There are a lot of children on Medicaid.”
Between the lines: Not all of the Medicaid enrollees who are removed from the program would become uninsured. But parents and their children could be headed down different paths if their household income has risen even slightly.
Adults who’ve returned to work may be able to get insurance through their employer. Others could get coverage through the ACA marketplace, though it’s unclear whether that would come the COVID-inspired extra financial assistance that’s now being offered.
Most kids would be headed for the Children’s Health Insurance Program, Alker said — a prospect that can entail added red tape and the payment of premiums or an annual enrollment fee, depending on the state.
What we’re watching: Changes in children’s coverage could be most pronounced in Texas, Florida and Georgia — the biggest non-Medicaid expansion states, which have higher rates of uninsured children than the national average.
Congress could still require continuous Medicaid coverage, the way the House did when it passed the sweeping social policy package that stalled in the Senate over cost concerns.
CMS’ Office of the Actuary projects a smaller decline in Medicaid enrollment than some health policy experts are predicting — and the Biden administration continues to move people deemed ineligible for Medicaid onto ACA plans, Raymond James analyst Chris Meekins noted in a recent report on the unwinding of the public health emergency.
Johnson & Johnson became the 16th drugmaker to limit 340B discounts for hospitals dispensing drugs at contract pharmacies. These manufacturers have taken issue with the proliferation of contract pharmacies in the 340B program, alleging high rates of fraud and duplicative billing. Several court battles between these drug companies and the federal government are ongoing.
The 340B program, which requires pharmaceutical companies to provide 20 to 50 percent discounts for drugs participating hospitals purchase (see our explainer on the mechanics of the program here), has grown rapidly in recent years.
The Gist:Over 40 percent of hospitals now qualify for 340B discounts, and 340B drug sales totaled $38B in 2020. According to a recent survey, participating hospitals have lost 25 to 40 percent of their contract pharmacy savings since drugmakers began restricting discounts in 2020.
Many hospitals have used savings from the program to subsidize other areas of patient care; some tell us that losing 340B revenue would erase their entire margin. Health systems should plan for a future in which their bottom lines are not dependent on this increasingly at-risk revenue source.
Judging from our recent conversations with health system executives, we’d guess CEOs across the industry woke up this morning glad to see the first quarter in the rearview mirror.
Almost everyone we’ve spoken to has told us that the past three months have been miserable from an operating margin perspective—skyrocketing labor costs, rising drug and supply prices, and stubbornly long length of stay, particularly among Medicare patients.
In the words of one CFO, “I’ve never seen anything like this. For the first time, we budgeted for a negative margin, and still didn’t hit our target. I’m not sure how long our board will let us stay on this trajectory before things change.”
Yet few of the drivers of poor financial performance appear to be temporary. Perhaps the over-reliance on agency nursing staff will wane as COVID volumes bottom out (for how long remains unknown), but overall labor costs will remain high, there’s no immediate relief for supply chain issues, and COVID-related delays in care have left many patients sicker—and thus in need of more costly care. Plus, the lifeline of federal relief funds is rapidly dwindling, if not already gone.
Expect the next three quarters (and beyond) to bring a greater focus on cost cutting, especially as not-for-profit systems struggle to defend their bond ratings in the face of rising interest rates.
Even as COVID admissions continue to wane, hospitals report that workforce shortages persist. The impact on hospital finances is stark: as shown in the graphic above, there has beenan eight percent increase in clinical labor costs per patient day since the start of the pandemic, amounting to an additional $17M annually for an average 500-bed hospital.
Two of the primary factors driving this increase—higher turnover among clinical staff and a continued reliance on travel nurses—are mutually reinforcing.
Quarterly turnover rates for some nursing positions doubled from Q4 2019 to Q2 2021, as hospitals turned to expensive agency labor to fill resulting vacancies. Spiking demand for travel nurses, still running nearly three times higher than the pre-pandemic baseline, fueled more turnover, as more nurses left for these lucrative roles.
It’s unclear how long increased labor costs will persist.
Some HR tactics, like signing and retention bonuses, are one-time expenditures. But total hospital employment is still down two percent from pre-pandemic levels, pointing to a diminished healthcare labor supply.
Permanent wage increases may end up being unavoidable, especially for lower-wage jobs, where a new compensation baseline for talent is being set by the market, both inside and outside the healthcare industry.
Since the for-profit system acquired six-hospital, Asheville, NC-based Mission Health in February 2019, there has been a series of reports about cascading community impacts, including a large physician exodus from the system. Local news outlet Asheville Watchdog counts 223 doctors who are no longer included in the system’s online directory, which currently lists about 1,600 physicians; HCA has also reportedly reduced health system staff by over 12 percent since the acquisition. Former Mission doctors say that patient care at the system is suffering, and that HCA doesn’t place the same value on primary care that Mission Health physicians historically did.
The Gist:The cultural shift from 130 years as a nonprofit community fixture to for-profit health system subsidiary has been rocky for Mission. Even before the HCA deal had been finalized, Mission physicians expressed concerns about how the company would implement its lean staffing and operational “playbook”. These expected changes were surely compounded by COVID-related staffing challenges.
Physician stakeholders who feel uncertain about the impact of an impending merger can sometimes use their voice to stymie health system combinations (see Beaumont Health’s failed merger with Advocate Aurora Health), but may alsovote with their feet when dissatisfied with new ownership, leaving critical gaps in patient care.