Starting next month, the federal government will stop reimbursing hospitals and other providers for the vaccination, testing, and treatment of uninsured COVID-19 patients. So far, about 50K providers have submitted a total of $20B of claims for COVID-related care for the uninsured.
Congress has yet to authorize more funding for this and other COVID relief programs, after stripping $15.6B from the latest government spending package. Though the White House is asking Congress to authorize $22.5B for further COVID aid and surge preparedness, it’s not clear how much of any new funding would go toward reimbursing care for the uninsured.
The Gist: This news comes as US officials expect a rise in cases driven by the Omicron BA.2 subvariant. Hospitals, already struggling with high labor and supply expenses, will face further margin pressures if a future COVID surge brings increased hospitalizations.
This will be especially true for safety net hospitals, and for those in states which haven’t expanded Medicaid. At the same time, 15M Americans are also at risk of losing Medicaid coverage when the federal government ends the public health emergency. Lower-income patients and the hospitals that treat them have already shouldered COVID’s worst effects, and the funding stalemate risks further worsening their situation.
Obamacare enrollment at a record-high 14.5 million
Congress may not fund premium subsidies in 2023
The Affordable Care Act marks its 12th anniversary Wednesday, and despite a record 14.5 million enrollees, the Biden administration is preparing for the possibility that millions could lose coverage next year.
The $1.9 trillion pandemic stimulus package (Public Law 117-2), signed March 2021, reduced Obamacare premiums to no more than 8.5% of income for eligible households and expanded premium subsidies to households earning more than 400% of the federal poverty level. The rescue plan also provided additional subsidies to help with out-of-pocket costs for low-income people. As a result, 2.8 million more consumers are receiving tax credits in 2022 compared to 2021.
But without congressional action, the subsidies—and the marketplace enrollment spikes they ushered in—could be lost in 2023. A new HHS report released Wednesday, shows an estimated 3.4 million Americans would lose marketplace coverage and become uninsured if the premium tax credits aren’t extended beyond 2022.
In a briefing with reporters Tuesday, Chiquita Brooks-LaSure, administrator for the Centers for Medicare & Medicaid Services, said her agency is “confident that Congress will really understand how important the subsidies were” to enrolling more people this year. The CMS would “pivot quickly,” however, to implement new policies and outreach plans if the subsidies aren’t extended as open enrollment for 2023 begins in November.
“That said, today and tomorrow we are celebrating the Affordable Care Act,” Brooks-LaSure added. “As part of that process, we’ve been reminding ourselves that sometimes it takes some time to pass legislation. And just like the Affordable Care Act took time, we’re confident that Congress is going to address these critical needs for the American people.”
After years of legal and political brawls that turned the landmark legislation into a political football, Obamacare “is at its strongest point ever,” Brooks-LaSure said. The 14.5 million total enrollees—those who extended coverage and those who signed up for the first time—is a 21% increase from last year. The number of new consumers during the 2022 open enrollment period increased by 20% to 3.1 million from 2.5 million in 2021.
This week, the Department of Health and Human Services will highlight the impact of the ACA and the Biden administration’s efforts to strengthen the law. The CMS recently announced a new special enrollment period opportunity for people with household incomes under 150% of the federal poverty level who are eligible for premium tax credits. The new special enrollment period will make it easier for low-income people to enroll in coverage throughout the year.
Troubled times could be around the corner, however, as millions of people with Medicaid coverage could become uninsured after the public health emergency ends. Under the Families First Coronavirus Response Act (Public Law 116-127), signed March 2020, states must maintain existing Medicaid enrollment until the end of the month that the public health emergency is lifted. Once the continuous enrollment mandate ends, states will resume Medicaid redeterminations and disenrollments for people who no longer meet the program’s requirements.
Dan Tsai, deputy administrator and director of the Center for Medicaid and CHIP Services at CMS, said the agency is working with states to make sure people who lose Medicaid coverage can be transferred into low- and no-cost Obamacare coverage.
“A substantial portion of individuals who will no longer be eligible for Medicaid will be eligible for other forms of coverage,” including marketplace coverage, Tsai told reporters Tuesday.
In a statement, President Joe Biden acknowledged the law’s great impact. “This law is the reason we have protections for pre-existing conditions in America. It is why women can no longer be charged more simply because they are women. It reduced prescription drug costs for nearly 12 million seniors. It allows millions of Americans to get free preventive screenings, so they can catch cancer or heart disease early—saving countless lives. And it is the reason why parents can keep children on their insurance plans until they turn 26.”
A new spring brings another anniversary of the Affordable Care Act. Twelve (sometimes tumultuous) years later, this remarkably resilient law is on firmer ground than ever before.
And there are currently no existential legal threats to the law working their way through federal courts.
In some ways, this rosy report feels unremarkable. Why expect otherwise with the law now in place for more than a decade and baked into every part of the health care system?
But this outcome was far from inevitable.
Just five years ago, Congress tried to repeal as much of the law as possible. When those broader efforts failed, Congress eliminated the much-maligned individual mandate penalty. We appeared to have reached a stalemate: Democrats could not improve the law while Republicans could not repeal it.
Could this be the moment we moved on from ACA politics?!
Enter the courts. In early 2018, Republican attorneys general sued to invalidate the mandate and, with it, the rest of the law. That lawsuit—California v. Texas—was ultimately heard by a new Supreme Court one week after the 2020 election, and the ACA was upheld just last summer.
This marked the third time that the Supreme Court largely rebuffed what could have been a crippling legal challenge to the law. It feels like ancient history now, but it is worth remembering that we were still playing “will they or won’t they?” with the Supreme Court and ACA only one year ago.
In the meantime, the Trump administration tried to undermine access to coverage under the law—except when it didn’t. I won’t list all the relevant Trump-era policies, but they had an impact: the uninsured rate rose, and marketplace enrollment declined until the 2021 plan year.
Ironically, one policy meant to destabilize the market had the opposite effect: so-called “silver loading” led to more generous marketplace subsidies and likely helped stave off even greater coverage losses.
This is the recent history that is top of mind as I reflect on the year ahead—and the work left to do to achieve universal coverage. Here are just some of the major issues facing policymakers:
• The clock is ticking toextend the American Rescue Plan Act subsidies. If Congress fails to do so, millions will face premium hikes next year and marketplace enrollment will likely drop.
• More than 2 million low-income peopleremain stuck in the Medicaid coverage gap in the 12 states that have not yet expanded their Medicaid program.
• Up to 15 million people, including nearly 6 million children, could lose Medicaid coverage at the end of the COVID-19 public health emergency.
• There is increasingly an affordability and underinsurance crisis, including for those with job-based coverage: an estimated 87 million peoplewere underinsured in 2018.
Congress and the White House are working to address these challenges, but much uncertainty remains.
“It feels like ancient history now, but it is worth remembering that we were still playing ‘will they or won’t they?’ with the Supreme Court and Affordable Care Act only one year ago.” – Katie Keith
Looking beyond Congress, 2022 will be an important year for regulatory changes. The Biden administration has proposed, but has not yet finalized, major marketplace changes. Other already-identified priorities include fixing the family glitch, limiting short-term limited duration insurance, and enhancing nondiscrimination protections. We could see movement on at least some of these rules soon.
While the Biden administration may be waiting out Congress before initiating some rulemaking, time is of the essence. New rules take many months to adopt and then take effect—followed by more time to deal with the legal challenges that typically follow.
Follow along as I dive deep on these issues and more in a new Health Affairs’ Health Reform newsletter.
We’ll highlight the latest health policy developments—from legislation to litigation—and explain what these changes mean for patients, payers, providers, and other key health care stakeholders.
It’s Your Birthday, Affordable Care Act!
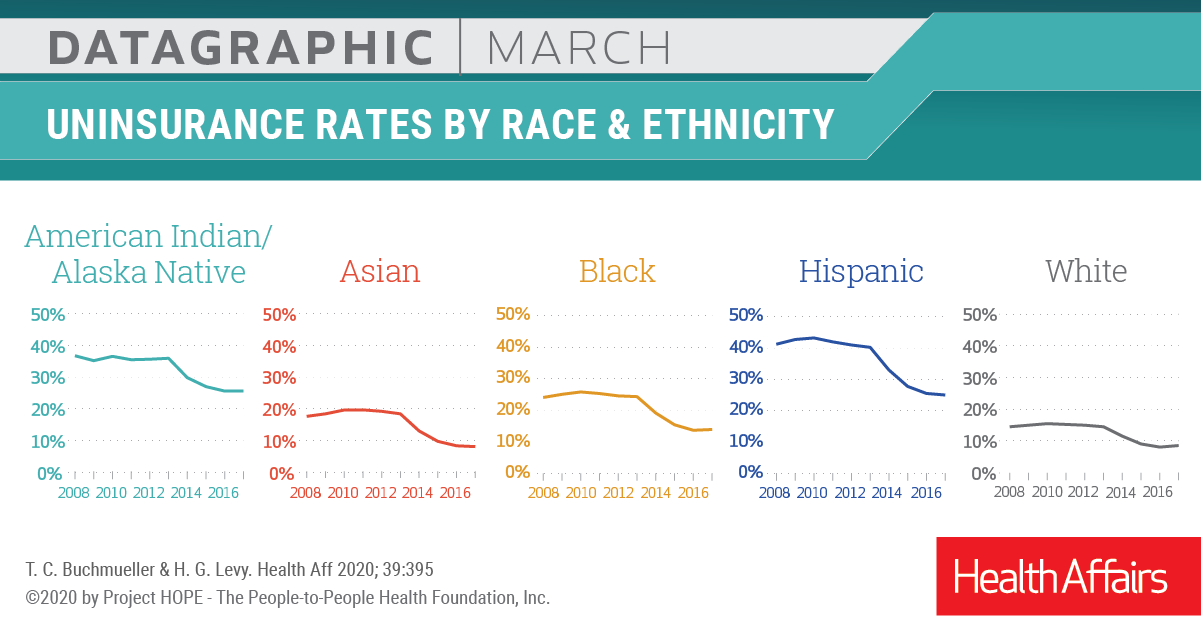
In March 2020, Health Affairspublished a theme issue to celebrate the tenth anniversary of the Affordable Care Act. The issue contains many illuminating research articles on the landmark legislation, from its impact on “the cost curve” to Medicaid expansion.
Above is a datagraphic from the issue showing how the ACA affected insurance coverage.
Insurers, retailers, and other healthcare companies vastly exceed health system scale, dwarfing even the largest hospital systems. The graphic above illustrates how the largest “mega-systems” lag other healthcare industry giants, in terms of gross annual revenue.
Amazon and Walmart, retail behemoths that continue to elbow into the healthcare space, posted 2021 revenue that more than quintuples that of the largest health system, Kaiser Permanente. The largest health systems reported increased year-over-year revenue in 2021, largely driven by higher volumes, as elective procedures recovered from the previous year’s dip.
However, according to a recent Kaufman Hall report, while health systems, on average, grew topline revenue by 15 percent year-over-year, they face rising expenses, and have yet to return to pre-pandemic operating margins.
Meanwhile, the larger companies depicted above, including Walmart, Amazon, CVS Health, and UnitedHealth Group, are emerging from the pandemic in a position of financial strength, and continue to double down on vertical integration strategies, configuring an array of healthcare assets into platform businesses focused on delivering value directly to consumers.
A National Bureau of Economic Research working paper found that higher-priced hospitals in competitive markets were associated with lower patient mortality—flying in the face of the common policy narrative that higher-priced care is not higher quality. However, in more concentrated, less-competitive healthcare markets (in which over two-thirds of the nation’s hospitals are located), the study found no correlation between price and quality. Authors of the study analyzed patient outcomes from more than 200K admissions among commercially insured patients, transported by ambulance to about 1,800 hospitals between 2007 and 2014.
The Gist: As hospitals have consolidated, prices have risen by about 30 percent between 2015 to 2019, leading policy experts and regulators to search for ways to rein in price inflation.
While there continues to be widespread consensus that industry consolidation has resulted in unsustainable cost growth, the new study’s findings bring a bit of welcome nuance around impact on quality and outcomes to an otherwise one-sided, price-centric policy narrative.
The US healthcare sector added 64K jobs in February, an increase from recent months, but the gains were concentrated in provider offices and home health companies. Hospitals and nursing facilities, which have both struggled with widespread staffing shortages, saw more anemic job growth. In particular, nursing homes have lost 15 percent of their workforce, remaining significantly understaffed even though resident occupancy rates still lag pre-pandemic levels. This week, nursing home groups pushed back against President Biden’s call for minimum staffing levels, calling them unrealistic without federal funding.
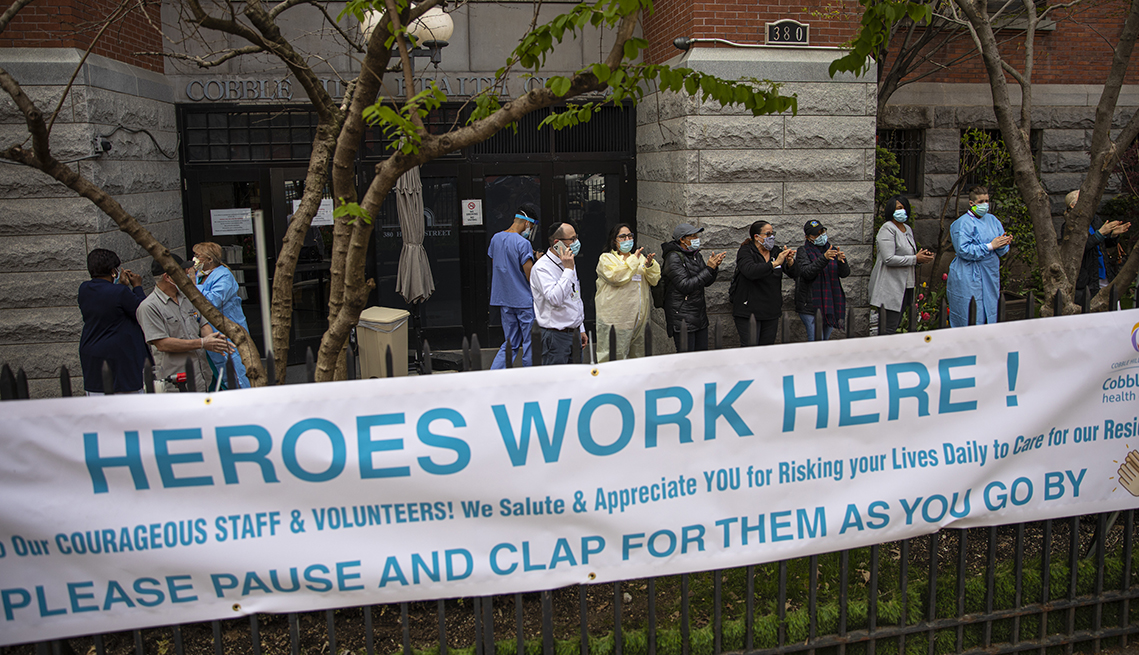
The Gist: Hospital and nursing facility workers have taken on some of the most taxing and dangerous jobs during the pandemic, caring for the sickest patients while personally risking COVID infection.
Healthcare workers are increasingly opting for safer, less intense jobs in outpatient care settings like physician offices, or are exiting direct patient care entirely. Even as the pandemic subsides, recruitment and retention of nurses and other caregivers will be of paramount importance, given rising vacancy rates and unabating staff shortages.
While many hospitals face financial hardships and rising expenses from the COVID-19 pandemic, several large health systems ended 2021 with profits above $1 billion.
These big health systems attributed the financial performance to several factors, including bigger investment gains and higher-acuity patients.
Seven health systems that posted net income of $1 billion last year:
1. Pittsburgh-based UPMC, an integrated delivery system with 40 hospitals, recorded a net income of $1.1 billion in 2021, driven by an operating income of $843 million and nonoperating gains of $810 million.
2. AdventHealth, a 48-hospital system based in Altamonte Springs, Fla., recorded a net income of $1.5 billion in 2021. The net income included an operating income of $994.6 million and investment gains of $517.7 million. In 2020, the health system’s net income was $914.8 million.
3. Cleveland Clinicreported a 66.7 percent increase in net income for the 12 months ended Dec. 31. The 19-hospital system saw its net income hit $2.2 billion, including an operating income of $746.3 million and investment gains of $1.4 billion.
4. Rochester, Minn.-based Mayo Clinic’s net income for 2021 was $3.6 billion, up from $2.5 billion a year earlier. The results included an operating income of $1.2 billion.
5. Driven by strong investment gains, Oakland, Calif.-based Kaiser Permanenterecorded a net income of $8.1 billion in 2021, an increase of $1.7 billion from 2020. The sharp rise in net income from the integrated delivery system with 39 hospitals included $7.5 billion in other income, including investment gains, and $611 million in operating income for 2021.
6. Nashville, Tenn.-based HCA Healthcare, a 182-hospital system, reported a net income of $7.7 billion in 2021, including investment gains and operating profits.
7. Tenet Healthcare, a 60-hospital system based in Dallas, reported net income of $1.5 billion on revenues of $19.5 billion in 2021. Tenet ended the 12-month period with an operating income of $2.9 billion, up from $2 billion recorded one year before. It also recorded losses on nonoperating activities and said its results for the year ending Dec. 31 included a pretax gain of $406 million associated with the divestiture of five Miami area hospitals, as well as stimulus funds totaling $205 million.
In our recent conversations with executives, we’ve heard that the workforce crisis continues to be the most urgent issue confronting health systems.
It’s a many-sided problem: early retirements hitting the nursing staff, leading to an overall loss of experience; early and mid-career nurses choosing to work for temporary staffing agencies for much higher pay, resulting in increased labor costs and resentment among remaining nurses; and a rising vacancy rate made more challenging by difficulty competing for talent against others offering higher pay and less stressful work environments.
But one factor undermining frontline nurse engagement hadn’t occurred to us, until we heard a chief nursing officer describe it this week. The lingering supply chain crisis is forcing hospitals to change where they purchase basic items—think IV tubing and bags, surgery kits, some basic drugs—which in turn forces nurses to adapt to using unfamiliar supplies on the fly, making for a less predictable work environment. On a busy and staff-constrained nursing unit, even small changes to standard procedures can be incredibly frustrating for nurses, and even lead to patient safety issues. Just another way in which the current environment is creating unprecedented pressure on healthcare workers, with little prospect for improvement anytime soon.
Healthcare professionals in Oklahoma who have cared for COVID-19 patients throughout the pandemic are now facing a facility lockdown due to threats made against them.
Mercy Hospital Oklahoma City upped its security and locked down its intensive care unit following online threats against the facility and its staff, mostly revolving around COVID treatments and conspiracy theories, Becker’s Hospital Review reported.
Claims made during a recent protest outside the facility and online included that the hospital had a “Fauci protocol,” and that it received government vouchers for using certain medications or treatments for COVID patients, which Mercy Hospital denied, according to Becker’s.
Hospital officials released a statement to staff on Friday, which they shared with MedPage Today. “There is truly nothing more important to us than your safety. We have a team monitoring these online attacks in real time. Every level of our ministry is deeply concerned and committed to doing whatever it takes to protect our co-workers against these baseless attacks,” they said.
“We are proud to serve with you,” they added. “We know you are tired and weary, but please try your best to put these baseless claims out of your mind. Remember, you are called to serve our patients and each other. We are praying for peace and protection over each of you, as well as the protection of all our patients and visitors, while we take action on your behalf.”
Late last week, the hospital filed a restraining order against the founder and director of an Oklahoma church group that has been protesting outside the facility and making threats against its staff online, Oklahoma’s KFOR reported.
In a recent press release, the church group, known as Ekklesia Oklahoma, called Mercy Hospital an “evil Marxist controlled death camp.”
Court documents stated that the founder of the group called one of the hospital’s doctors a “murderer,” noting that members even posted the doctor’s home address online, according to KFOR.
Hospital officials told KFOR that they are thankful for local police departments that are providing extra security for staff and patients.
Other hospitals across the U.S. have also received threats to the safety of healthcare workers in recent days.
Last week, the Massachusetts Medical Society said it was “angered” over the recent neo-Nazi protest outside Brigham and Women’s Hospital in Boston that targeted two doctors whose work focuses on health equity.
Carole Allen, MD, MBA, president of the society, told MedPage Today that the protest outside Brigham and Women’s was a threat to healthcare workers who were just trying to do their jobs, as well as to patients, and was so disruptive that it “could endanger healthcare in general.”
House Republicans are demanding the Biden administration starts winding down the COVID-19 public health emergency, while hospital lobbying groups are pressing it to do the opposite.
A group of more than 70 House Republicans wrote Thursday to Department of Health and Human Services (HHS) Secretary Xavier Becerra asking to start the process to wind down the COVID-19 public health emergency (PHE), which was recently extended until April. At the same time, several hospital advocacy groups are hoping the agency keeps the PHE beyond this spring and wants a 60-day notice as to when it will end.
“Although the PHE was certainly necessary at the outset of the pandemic, it was always meant to be temporary,” according to the GOP letter led by Rep. Cathy McMorris Rodgers, R-Washington, ranking member of the House Energy and Commerce Committee.
Republicans want HHS to release a concrete timeline for when the agency plans to exit the PHE.
“We recognize that the PHE cannot end overnight, and that certain actions must be taken to avoid significant disruption to patients and healthcare providers, including working with Congress to extend certain policies like maintaining access to telehealth services for our nation’s seniors,” the letter added.
The PHE granted major flexibilities for providers to get reimbursed by Medicare for telehealth, but those powers will go away after the PHE. It also gave flexibility on several reporting requirements and eased other regulatory burdens.
Another major issue is that states are going to be able to start eligibility redeterminations for Medicaid, which have been paused since the PHE went into effect in January 2020. State Medicaid directors are seeking a heads-up on when the emergency will go away, as states can start to disenroll ineligible beneficiaries after the PHE expires.
Republicans also want Becerra to cite any programs that should be made permanent, and they want “swift action” to lift all COVID-19 vaccine mandates.
The Supreme Court upheld the Biden administration’s healthcare worker vaccine mandate, overturning a lower court’s stay that affected half of the country. The Centers for Medicare & Medicaid Services has deadlines for states to comply with the vaccination mandate, and facilities that don’t fully comply could risk losing participation in Medicare and Medicaid.
The Republicans charge that the mandates have not “stopped the spread of COVID-19 but have alienated many Americans and have caused staff shortages at hospitals and other healthcare facilities.”
Key drivers of the staff shortages, however, have been a massive surge of the virus overwhelming facilities caused by the omicron variant along with increased expenses facilities have faced for temporary nursing staff. Those lingering expenses are the reason hospital groups are pressing for HHS to do the opposite and extend the PHE beyond April.
The Federation of American Hospitals (FAH) also wrote to Becerra Thursday (PDF) seeking to continue to extend the PHE “well beyond its current expiration date in April 2022.” Even though the omicron surge appears to be easing, the virus is still creating major operational challenges for providers, FAH said.
It also wants the administration to give hospitals a 60-day heads-up when it plans to end the PHE.
“Unwinding the complex web of PHE waiver-authorized operations, programs and procedures—which will have been in place and relied on for more than two years—is a major undertaking that, if rushed, risks destabilizing fragile healthcare networks that patients rely on for care,” the letter said.
The American Hospital Association also wrote to congressional leaders Tuesday seeking for more relief from Congress to help systems overcome staffing shortages that have exacerbated due to the omicron surge.
“The financial pressures hospitals and health systems faced at the beginning of the public health emergency continue, with, for example, ongoing delays in non-emergent procedures, in addition to increased expenses for supplies, medicine, testing and protective equipment,” the letter said.
FAH President Chip Kahn told Fierce Healthcare on Friday that the issues Republicans address in the letter are different from the priorities of the FAH, namely that the association doesn’t focus on mask or vaccine mandates.
“What we are saying is that the PHE has many aspects to it, and so … we think [it] should be extended, but if you don’t then we need to have a lengthy or carefully thought through transition,” Kahn said.
He added that Becerra’s predecessor, acting Secretary Eric Hargan, told providers that they would get a 60-day notice before the end of the PHE. That deadline for such a 60-day notice is Feb. 15.
Kahn said he understands the administration may be under political pressure to end the emergency, but prior notice is absolutely needed.
“I don’t know how they will respond but if they do choose to pull out, we just want to make sure that it doesn’t leave anything behind,” he said.