Many Americans, even those who don’t pay much attention to investing and the markets, know the name Warren Buffett.
Buffett, of course, is the billionaire philanthropist who created one of the greatest investment fortunes in history. Far fewer, however, know the name of his longtime business partner Charlie Munger.
And that’s a shame, because Munger is at least half the brains behind Berkshire Hathaway BRK.ABRK.B, the holding company he runs with Buffett and which manages billions and billions of investor dollars.
Munger turned 98 on Jan. 1. To celebrate his wit and market wisdom, here is a collection of quips from various interviews and question-and-answer sessions over the years.
On business education
Those of you who are about to enter business school, or who are there, I recommend you learn to do it our way. But at least until you’re out of school you have to pretend to do it their way.
On common sense
If people weren’t so often wrong, we wouldn’t be so rich.
On company earnings
Yeah, I think you would understand any presentation using the word EBITDA, if every time you saw that word you just substituted the phrase “bullsh** earnings.”
On a changing economy
So no, I’m optimistic about life. If I can be optimistic when I’m nearly dead, surely the rest of you can handle a little inflation.
On public spending
Everybody wants fiscal virtue but not quite yet. They’re like that guy who felt that way about sex. He was willing to give it up but not quite yet.
On legacy
Well, you don’t want to be like the motion picture executive in California. They said the funeral was so large because everybody wanted to make sure he was dead.
On stock buybacks
I think some people just buy it to keep the stock up. And that, of course, is insane. And immoral. But apart from that, it’s fine.
On marriage
Warren: Charlie is big on lowering expectations.
Munger: Absolutely. That’s the way I got married. My wife lowered her expectations.
On the purpose of money
Sure, there are a lot of things in life way more important than wealth. All that said…some people do get confused. I play golf with a man. He says: “What good is health? You can’t buy money with it.”
On money managers
The general system for money management requires people to pretend that they can do something that they can’t do, and to pretend to like it when they really don’t. I think that’s a terrible way to spend your life, but it’s very well paid.
On systematic investing
Well, I can’t give you a formulaic approach, because I don’t use one. If you want a formula you should go back to graduate school. They’ll give you lots of formulas that won’t work.
On human nature
As Samuel Johnson said, famously: “I can give you an argument, but I can’t give you an understanding.”
On financial innovation
It’s perfectly obvious, at least to me, that to say that derivative accounting in America is a sewer. is an insult to sewage.
On business competition
Competency is a relative concept. And what a lot of us needed to get ahead was to compete against idiots. And luckily there’s a large supply.
On cryptocurrency
I think the people who are professional traders that go into trading cryptocurrencies, it’s just disgusting. It’s like somebody else is trading turds and you decide, “I can’t be left out.”
On investment bankers
Once I asked a man who just left a large investment bank, and I said, “How does your firm make its money?” He said, “Off the top, off the bottom, off both sides, and in the middle.”
Over the past two years, historians and analysts have compared the coronavirus to the 1918 flu pandemic. Many of the mitigation practices used to combat the spread of the coronavirus, especially before the development of the vaccines, have been the same as those used in 1918 and 1919 — masks and hygiene, social distancing, ventilation, limits on gatherings (particularly indoors), quarantines, mandates, closure policies and more.
Yet, it may be that only now, in the winter of 2022, when Americans are exhausted with these mitigation methods, that a comparison to the 1918 pandemic is most apt.
The highly contagious omicron variant has rendered vaccines much less effective at preventing infections, thus producing skyrocketing caseloads. And that creates a direct parallel with the fall of 1918, which provides lessons for making January as painless as possible.
In February and March 1918, an infectious flu emerged. It spread from Kansas, through World War I troop and material transports, filling military post hospitals and traveling across the Atlantic and around the world within six months. Cramped quarters and wartime transport and industry generated optimal conditions for the flu to spread, and so, too, did the worldwide nature of commerce and connection. But there was a silver lining: Mortality rates were very low.
In part because of press censorship of anything that might undermine the war effort, many dismissed the flu as a “three-day fever,” perhaps merely a heavy cold, or simply another case of the grippe (an old-fashioned word for the flu).
Downplaying the flu led to high infection rates, which increased the odds of mutations. And in the summer of 1918, a more infectious variant emerged. In August and September, U.S. and British intelligence officers observed outbreaks in Switzerland and northern Europe, writing home with warnings that went largely unheeded.
Unsurprisingly then, this seemingly more infectious, much more deadly variant of H1N1 traveled west across the Atlantic, producing the worst period of the pandemic in October 1918. Nearly 200,000 Americans died that month. After a superspreading Liberty Loan parade at the end of September, Philadelphia became an epicenter of the outbreak. At its peak, nearly 700 Philadelphians died per day.
Once spread had begun, mitigation methods such as closures, distancing, mask-wearing and isolating those infected couldn’t stop it, but they did save many lives and limited suffering by slowing infections and spread. The places that fared best implemented proactive restrictions early; they kept them in place until infections and hospitalizations were way down, then opened up gradually, with preparations to reimpose measures if spread returned or rates elevated, often ignoring the pleas of special interests lobbying hard for a complete reopening.
In places in the United States where officials gave in to public fatigue and lobbying to remove mitigation methods, winter surges struck. Although down from October’s highs, these surges were still usually far worse than those in the cities and regions that held steady.
In Denver, in late November 1918, an “amusement” lobby — businesses and leaders invested in keeping theaters, movie houses, pool halls and other public venues open — successfully pressured the mayor and public health officials to rescind and then revise a closure order. This, in turn, generated what the Rocky Mountain News called “almost indescribable confusion,” followed by widespread public defiance of mask and other public health prescriptions.
In San Francisco, where resistance was generally less successful than in Denver, there was significant buy-in for a second round of masking and public health mandates in early 1919 during a new surge. But opposition created an issue. An Anti-Mask League formed, and public defiance became more pronounced. Eventually anti-maskers and an improving epidemic situation combined to end the “masked” city’s second round of mask and public health mandates.
The takeaway: Fatigue and removing mitigation methods made things worse. Public officials needed to safeguard the public good, even if that meant unpopular moves.
The flu burned through vulnerable populations, but by late winter and early spring 1919, deaths and infections dropped rapidly, shifting toward an endemic moment — the flu would remain present, but less deadly and dangerous.
Overall, nearly 675,000 Americans died during the 1918-19 flu pandemic, the majority during the second wave in the autumn of 1918. That was 1 in roughly 152 Americans (with a case fatality rate of about 2.5 percent). Worldwide estimates differ, but on the order of 50 million probably died in the flu pandemic.
In 2022, we have far greater biomedical and technological capacity enabling us to sequence mutations, understand the physics of aerosolization and develop vaccines at a rapid pace. We also have a far greater public health infrastructure than existed in 1918 and 1919. Even so, it remains incredibly hard to stop infectious diseases, particularly those transmitted by air. This is complicated further because many of those infected with the coronavirus are asymptomatic. And our world is even more interconnected than in 1918.
That is why, given the contagiousness of omicron, the lessons of the past are even more important today than they were a year ago. The new surge threatens to overwhelm our public health infrastructure, which is struggling after almost two years of fighting the pandemic. Hospitals are experiencing staff shortages (like in fall 1918). Testing remains problematic.
And ominously, as in the fall of 1918, Americans fatigued by restrictions and a seemingly endless pandemic are increasingly balking at following the guidance of public health professionals or questioning why their edicts have changed from earlier in the pandemic. They are taking actions that, at the very least, put more vulnerable people and the system as a whole at risk — often egged on by politicians and media figures downplaying the severity of the moment.
Public health officials also may be repeating the mistakes of the past. Conjuring echoes of Denver in late 1918, under pressure to prioritize keeping society open rather than focusing on limiting spread, the Centers for Disease Control and Prevention changed its isolation recommendations in late December. The new guidelines halved isolation time and do not require a negative test to reenter work or social gatherings.
Thankfully, we have an enormous advantage over 1918 that offers hope. Whereas efforts to develop a flu vaccine a century ago failed, the coronavirus vaccines developed in 2020 largely prevent severe illness or death from omicron, and the companies and researchers that produced them expect a booster shot tailored to omicron sometime in the winter or spring. So, too, we have antivirals and new treatments that are just becoming available, though in insufficient quantities for now.
Those lifesaving advantages, however, can only help as much as Americans embrace them. Only by getting vaccinated, including with booster shots, can Americans prevent the health-care system from being overwhelmed. But the vaccination rate in the country remains a relatively paltry 62 percent, and only a scant 1 in 5 have received a booster shot. And as in 1918, some of the choice rests with public officials. Though restrictions may not be popular, officials can reimpose them — offering public support where necessary to those for whom compliance would create hardship — and incentivize and mandate vaccines, taking advantage of our greater medical technology.
As the flu waned in 1919, one Portland, Ore., health official reflected that “the biggest thing we have had to fight in the influenza epidemic has been apathy, or perhaps the careless selfishness of the public.”
The same remains true today.
Vaccines, new treatments and century-old mitigation strategies such as masks, distancing and limits on gatherings give us a pathway to prevent the first six weeks of 2022 from being like the fall of 1918. And encouraging news about the severity of omicron provides real optimism that an endemic future — in which the coronavirus remains but poses far less of a threat — is near. The question is whether we get there with a maximum of pain or a minimum. The choice is ours.
Why are so many vaccinated people getting COVID-19 lately?
A couple of factors are at play, starting with the emergence of the highly contagious omicron variant. Omicron is more likely to infect people, even if it doesn’t make them very sick, and its surge coincided with the holiday travel season in many places.
People might mistakenly think the COVID-19 vaccines will completely block infection, but the shots are mainly designed to prevent severe illness, says Louis Mansky, a virus researcher at the University of Minnesota.
And the vaccines are still doing their job on that front, particularly for people who’ve gotten boosters.
Two doses of the Pfizer-BioNTech or Moderna vaccines or one dose of the Johnson & Johnson vaccine still offer strong protection against serious illness from omicron. While those initial doses aren’t very good at blocking omicron infection, boosters — particularly with the Pfizer and Moderna vaccines — rev up levels of the antibodies to help fend off infection.
Omicron appears to replicate much more efficiently than previous variants. And if infected people have high virus loads, there’s a greater likelihood they’ll pass it on to others, especially the unvaccinated. Vaccinated people who get the virus are more likely to have mild symptoms, if any, since the shots trigger multiple defenses in your immune system, making it much more difficult for omicron to slip past them all.
Advice for staying safe hasn’t changed. Doctors say to wear masks indoors, avoid crowds and get vaccinated and boosted. Even though the shots won’t always keep you from catching the virus, they’ll make it much more likely you stay alive and out of the hospital.
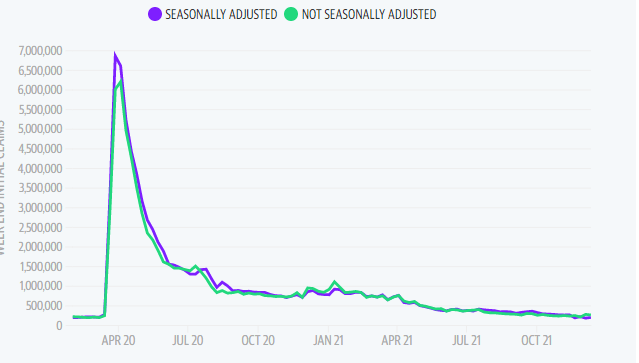
First-time unemployment filings fell by 8,000 claims from the previous week’s reading, marking the second lowest print during the pandemic and signaling continued recovery in the labor market as high demand for workers pours into the new year.
The Labor Department released its latest report on initial and continuing claims on Thursday at 8:30 a.m. ET. Here were the main metrics from the print, compared to consensus estimates compiled by Bloomberg:
Initial jobless claims, week ended Dec. 25: 198,000 vs. 206,000 expected and upwardly revised to 206,000 during prior week
Continuing claims, week ended Dec. 18: 1.716 million vs. 1.875 million expected and downwardly revised to 1.856 million during prior week
The newest print brings the four-week moving average to 199,300 in the week ending Dec. 25, Bloomberg data reflected. Continuing claims dropped to a fresh pandemic low of 1.716 million. Forecast for this week’s jobless claims release ranged from 190,000-225,000 from 22 economists surveyed by Bloomberg.
First-time filings for unemployment remained below the 2019 average of 218,000, when the unemployment rate was at a half-century low of 3.5%, according to Bloomberg. The current unemployment rate is also expected to edge down to 4.1% in December as the labor market continues to tighten.
At 205,000, last week’s initial unemployment claims were on par with economist forecasts and below pre-pandemic levels yet again. Earlier in December, jobless claims fell sharply to 188,000, the lowest level since 1969. The prints serve an early indication of the relative strength expected to show in December’s jobs report, though the economic impact of the virus remains unclear.
“Fortunately, there’s no evidence in this data of a new wave of fresh job loss,” Bankrate senior economic analyst Mark Hamrick said, commenting on last week’s figures. “New claims are only slightly above the lowest point in decades notched a couple of weeks ago.”
“With so much uncertainty now and the high level of concern about the Omicron variant, we’ll take stability when we can get it,” Hamrick added.
“It’s stunning to see how much the rate has fallen in the last five months,” he told Yahoo Finance Live. “We expect that pace of decline to slow, but it doesn’t take much to get below 4%, even with a tick up in the labor participation rate, which has been depressed over the last year and a half.”
Record cases of COVID-19 may discourage workers from looking for work as U.S. households continue to cite fear of COVID or virus-related caretaking needs as reasons for staying out of the job market.
“The pandemic’s resurgence is affecting the economy,” Hamrick said in a note last week. “The question is for how long and how much, and it is too early to know the answers.”