Moody’s Investors Service has downgraded the ratings on Providence’s revenue bond debt to “A1” from “Aa3.”
“The downgrade to ‘A1’ is driven by the disaffiliation with Hoag Hospital, and the expectation that weaker operating, balance sheet, and debt measures will continue for the time being,” Moody’s said in an April 5 release.
Renton, Wash.-based Providence and Newport Beach, Calif.-based Hoag ended their affiliation Jan. 31. The two organizations cut ties at a time when Providence is facing several challenges, including operating pressures, variable utilization and reliance on temporary labor, Moody’s said.
The “A1” rating and stable outlook also reflect Providence’s strengths, including a large service area, a large revenue base of more than $25 billion and a leading market share in all of its markets.
Moody’s said it expects Providence to continue to grow its operating platform and generate additional revenue growth.
Thousands of nurses at Stanford and Lucile Packard Children’s hospitals in Palo Alto, Calif., have authorized the union representing them to call a strike.
In an April 8 news release, the Committee for Recognition of Nursing Achievement said more than 4,500 nurses at Stanford and Packard, or 93 percent of all nurses eligible, voted in favor of strike authorization. They are calling on hospital management to adequately address staffing, citing consistent overtime and nurses’ complaints of inadequate resources, training or staff. They also seek improved access to mental health counseling, as well as competitive wages and benefits.
“The decision by members to overwhelmingly authorize a strike shows that we are fed up with the status quo of working conditions at the hospitals,” Colleen Borges, union president and a nurse in the pediatric oncology department, said in the release. “We need contracts that allow us to care for ourselves and our families so we can continue providing world-class care.”
Nurses authorized the strike after bargaining for the last 13 weeks and are working without contracts. The vote does not mean a strike will occur, but it gives the union the ability to issue an official strike notice.
In a statement shared with Becker’s, Stanford expressed its support for negotiations rather than a strike.
“We are committed, through good faith bargaining, to reach agreement on new contracts that provide nurses a highly competitive compensation package, along with proposals that further our commitment to enhancing staffing and wellness benefits for nurses,” the statement said.
The hospital also said it is taking the steps to prepare for the possibility of a strike, while hoping a strike is averted.
“Given the progress we have made by working constructively with the union, we should be able to reach agreements that will allow us to continue to attract and retain the high caliber of nurses who so meaningfully contribute to our hospitals’ reputation for excellence,” the statement read.
Hospitals across the U.S. saw their operating margins remain negative for the second consecutive month in February as they continued to feel the repercussions of the winter omicron surge, according to Kaufman Hall’s “National Hospital Flash Report: March 2022” posted March 28.
The median operating margin in February was -3.45 percent, up from -4.52 percent in January, but “still well below sustainable levels,” Kaufman Hall said.
Kaufman Hall said the improvement in hospital margin was driven by disproportionate increases among several hospitals that saw margin gains, but most hospitals reported margin declines in February. Specifically, the median operating margin was down 11.8 percent month over month.
“The second month of 2022 brought further challenges for the nation’s hospitals and health systems,” Kaufman Hall said. “Overall, the year is off to a difficult start.”
Kaufman Hall noted that patient days were down 13.3 percent month over month, and fewer severely ill COVID-19 patients also contributed to shorter hospital stays as the average length of stay dropped 5.3 percent month over month.
Hospitals’ gross operating revenue also decreased 7.4 percent compared to January 2022, with outpatient revenue falling 5 percent and inpatient revenue declining 19.3 percent.
Kaufman Hall noted that hospitals saw some improvement month over month in terms of expenses. Total expenses per adjusted discharge fell 4.5 percent compared to January, labor expense per adjusted discharge fell 6.1 percent and non-labor expenses per adjusted discharge was down 3.6 percent. However, Kaufman Hall noted that year over year, expenses are still up significantly, with total adjusted expense per adjusted discharge rising 10.4 percent compared to February 2021.
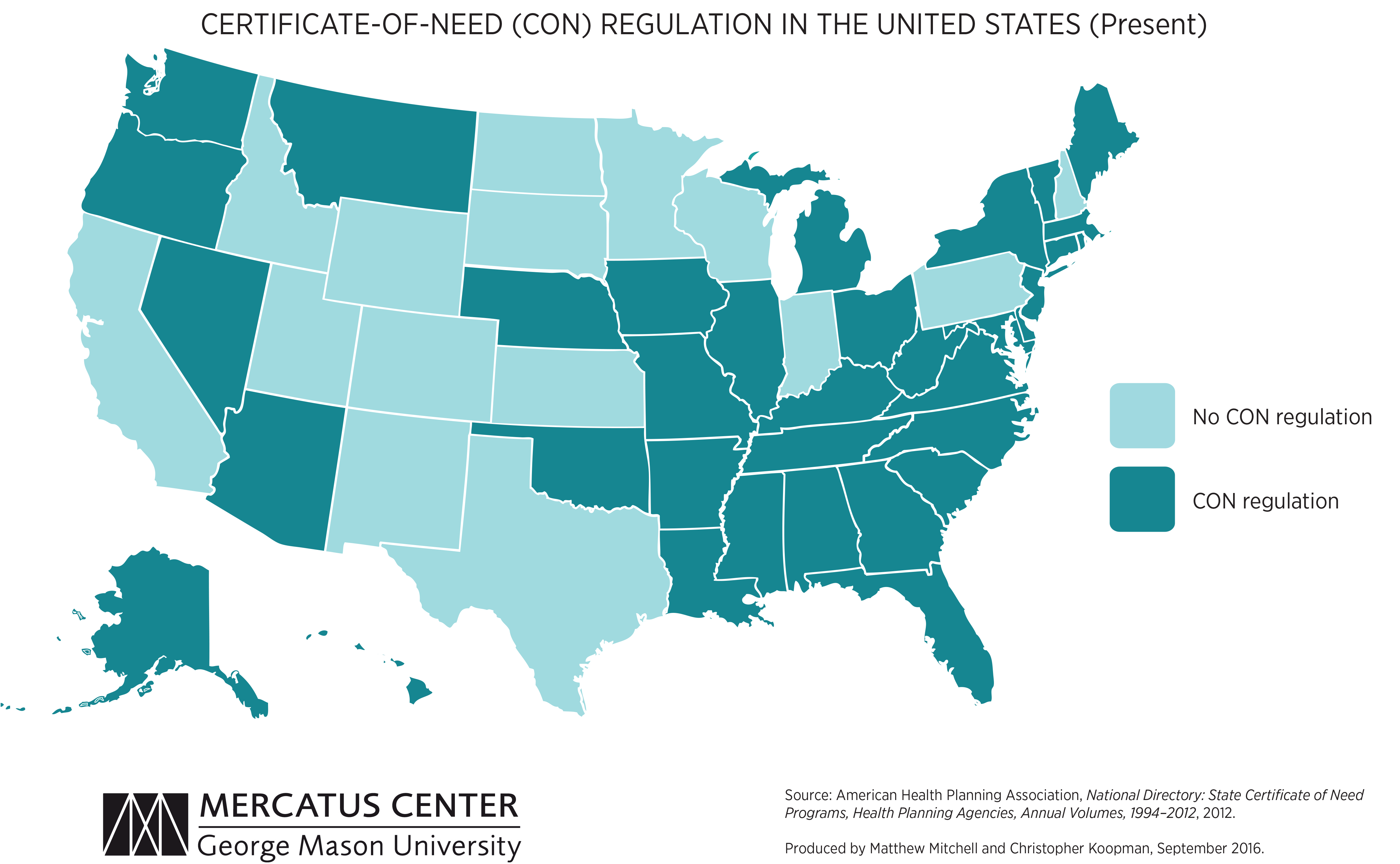
We’re picking up on a growing concern among health system leaders that many states with “certificate of need” (CON) laws in effect are on the cusp of repealing them. CON laws, currently in place in 35 states and the District of Columbia, require organizations that want to construct new or expand existing healthcare facilities to demonstrate community need for the additional capacity, and to obtain approval from state regulatory agencies. While the intent of these laws is to prevent duplicative capacity, reduce unnecessary utilization, and control cost growth, critics claim that CON requirements reduce competition—and free market-minded state legislators, particularly in the South and Midwest, have made them a target.
One of our member systems located in a state where repeal is being debated asked us to facilitate a scenario planning session around CON repeal with system and physician leaders. Executives predicted that key specialty physician groups would quickly move to build their own ambulatory surgery centers, accelerating shift of surgical volume away from the hospital.
The opportunity to expand outpatient procedure and long-term care capacity would also fuel investment from private equity, which have already been picking up in the market. An out-of-market health system might look to build microhospitals, or even a full-service inpatient facility, which would be even more disruptive.
CON repeal wasn’t all downside, however; the team identified adjacent markets they would look to enter as well. The takeaway from our exercise: in addition to the traditional response of flexing lobbying influence to shape legislative change, the system must begin to deliver solutions to consumers that are comprehensive, convenient, and competitively priced—the kind of offerings that might flood the market if CON laws were lifted.
Starting next month, the federal government will stop reimbursing hospitals and other providers for the vaccination, testing, and treatment of uninsured COVID-19 patients. So far, about 50K providers have submitted a total of $20B of claims for COVID-related care for the uninsured.
Congress has yet to authorize more funding for this and other COVID relief programs, after stripping $15.6B from the latest government spending package. Though the White House is asking Congress to authorize $22.5B for further COVID aid and surge preparedness, it’s not clear how much of any new funding would go toward reimbursing care for the uninsured.
The Gist: This news comes as US officials expect a rise in cases driven by the Omicron BA.2 subvariant. Hospitals, already struggling with high labor and supply expenses, will face further margin pressures if a future COVID surge brings increased hospitalizations.
This will be especially true for safety net hospitals, and for those in states which haven’t expanded Medicaid. At the same time, 15M Americans are also at risk of losing Medicaid coverage when the federal government ends the public health emergency. Lower-income patients and the hospitals that treat them have already shouldered COVID’s worst effects, and the funding stalemate risks further worsening their situation.
Obamacare enrollment at a record-high 14.5 million
Congress may not fund premium subsidies in 2023
The Affordable Care Act marks its 12th anniversary Wednesday, and despite a record 14.5 million enrollees, the Biden administration is preparing for the possibility that millions could lose coverage next year.
The $1.9 trillion pandemic stimulus package (Public Law 117-2), signed March 2021, reduced Obamacare premiums to no more than 8.5% of income for eligible households and expanded premium subsidies to households earning more than 400% of the federal poverty level. The rescue plan also provided additional subsidies to help with out-of-pocket costs for low-income people. As a result, 2.8 million more consumers are receiving tax credits in 2022 compared to 2021.
But without congressional action, the subsidies—and the marketplace enrollment spikes they ushered in—could be lost in 2023. A new HHS report released Wednesday, shows an estimated 3.4 million Americans would lose marketplace coverage and become uninsured if the premium tax credits aren’t extended beyond 2022.
In a briefing with reporters Tuesday, Chiquita Brooks-LaSure, administrator for the Centers for Medicare & Medicaid Services, said her agency is “confident that Congress will really understand how important the subsidies were” to enrolling more people this year. The CMS would “pivot quickly,” however, to implement new policies and outreach plans if the subsidies aren’t extended as open enrollment for 2023 begins in November.
“That said, today and tomorrow we are celebrating the Affordable Care Act,” Brooks-LaSure added. “As part of that process, we’ve been reminding ourselves that sometimes it takes some time to pass legislation. And just like the Affordable Care Act took time, we’re confident that Congress is going to address these critical needs for the American people.”
After years of legal and political brawls that turned the landmark legislation into a political football, Obamacare “is at its strongest point ever,” Brooks-LaSure said. The 14.5 million total enrollees—those who extended coverage and those who signed up for the first time—is a 21% increase from last year. The number of new consumers during the 2022 open enrollment period increased by 20% to 3.1 million from 2.5 million in 2021.
This week, the Department of Health and Human Services will highlight the impact of the ACA and the Biden administration’s efforts to strengthen the law. The CMS recently announced a new special enrollment period opportunity for people with household incomes under 150% of the federal poverty level who are eligible for premium tax credits. The new special enrollment period will make it easier for low-income people to enroll in coverage throughout the year.
Troubled times could be around the corner, however, as millions of people with Medicaid coverage could become uninsured after the public health emergency ends. Under the Families First Coronavirus Response Act (Public Law 116-127), signed March 2020, states must maintain existing Medicaid enrollment until the end of the month that the public health emergency is lifted. Once the continuous enrollment mandate ends, states will resume Medicaid redeterminations and disenrollments for people who no longer meet the program’s requirements.
Dan Tsai, deputy administrator and director of the Center for Medicaid and CHIP Services at CMS, said the agency is working with states to make sure people who lose Medicaid coverage can be transferred into low- and no-cost Obamacare coverage.
“A substantial portion of individuals who will no longer be eligible for Medicaid will be eligible for other forms of coverage,” including marketplace coverage, Tsai told reporters Tuesday.
In a statement, President Joe Biden acknowledged the law’s great impact. “This law is the reason we have protections for pre-existing conditions in America. It is why women can no longer be charged more simply because they are women. It reduced prescription drug costs for nearly 12 million seniors. It allows millions of Americans to get free preventive screenings, so they can catch cancer or heart disease early—saving countless lives. And it is the reason why parents can keep children on their insurance plans until they turn 26.”
A new spring brings another anniversary of the Affordable Care Act. Twelve (sometimes tumultuous) years later, this remarkably resilient law is on firmer ground than ever before.
And there are currently no existential legal threats to the law working their way through federal courts.
In some ways, this rosy report feels unremarkable. Why expect otherwise with the law now in place for more than a decade and baked into every part of the health care system?
But this outcome was far from inevitable.
Just five years ago, Congress tried to repeal as much of the law as possible. When those broader efforts failed, Congress eliminated the much-maligned individual mandate penalty. We appeared to have reached a stalemate: Democrats could not improve the law while Republicans could not repeal it.
Could this be the moment we moved on from ACA politics?!
Enter the courts. In early 2018, Republican attorneys general sued to invalidate the mandate and, with it, the rest of the law. That lawsuit—California v. Texas—was ultimately heard by a new Supreme Court one week after the 2020 election, and the ACA was upheld just last summer.
This marked the third time that the Supreme Court largely rebuffed what could have been a crippling legal challenge to the law. It feels like ancient history now, but it is worth remembering that we were still playing “will they or won’t they?” with the Supreme Court and ACA only one year ago.
In the meantime, the Trump administration tried to undermine access to coverage under the law—except when it didn’t. I won’t list all the relevant Trump-era policies, but they had an impact: the uninsured rate rose, and marketplace enrollment declined until the 2021 plan year.
Ironically, one policy meant to destabilize the market had the opposite effect: so-called “silver loading” led to more generous marketplace subsidies and likely helped stave off even greater coverage losses.
This is the recent history that is top of mind as I reflect on the year ahead—and the work left to do to achieve universal coverage. Here are just some of the major issues facing policymakers:
• The clock is ticking toextend the American Rescue Plan Act subsidies. If Congress fails to do so, millions will face premium hikes next year and marketplace enrollment will likely drop.
• More than 2 million low-income peopleremain stuck in the Medicaid coverage gap in the 12 states that have not yet expanded their Medicaid program.
• Up to 15 million people, including nearly 6 million children, could lose Medicaid coverage at the end of the COVID-19 public health emergency.
• There is increasingly an affordability and underinsurance crisis, including for those with job-based coverage: an estimated 87 million peoplewere underinsured in 2018.
Congress and the White House are working to address these challenges, but much uncertainty remains.
“It feels like ancient history now, but it is worth remembering that we were still playing ‘will they or won’t they?’ with the Supreme Court and Affordable Care Act only one year ago.” – Katie Keith
Looking beyond Congress, 2022 will be an important year for regulatory changes. The Biden administration has proposed, but has not yet finalized, major marketplace changes. Other already-identified priorities include fixing the family glitch, limiting short-term limited duration insurance, and enhancing nondiscrimination protections. We could see movement on at least some of these rules soon.
While the Biden administration may be waiting out Congress before initiating some rulemaking, time is of the essence. New rules take many months to adopt and then take effect—followed by more time to deal with the legal challenges that typically follow.
Follow along as I dive deep on these issues and more in a new Health Affairs’ Health Reform newsletter.
We’ll highlight the latest health policy developments—from legislation to litigation—and explain what these changes mean for patients, payers, providers, and other key health care stakeholders.
It’s Your Birthday, Affordable Care Act!
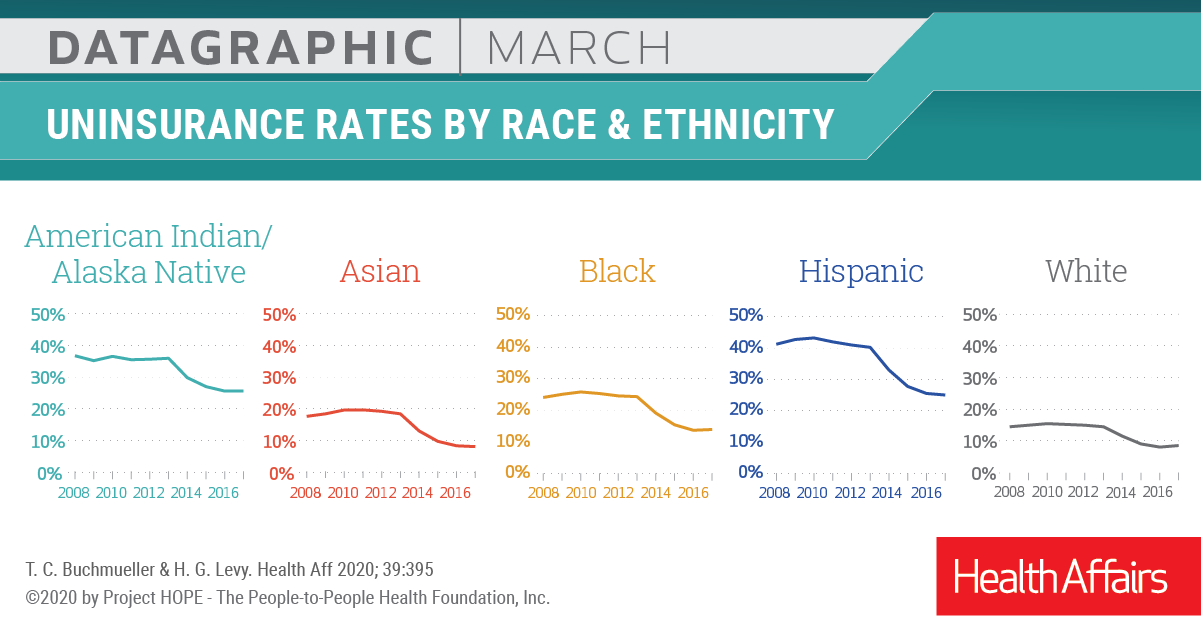
In March 2020, Health Affairspublished a theme issue to celebrate the tenth anniversary of the Affordable Care Act. The issue contains many illuminating research articles on the landmark legislation, from its impact on “the cost curve” to Medicaid expansion.
Above is a datagraphic from the issue showing how the ACA affected insurance coverage.
Insurers, retailers, and other healthcare companies vastly exceed health system scale, dwarfing even the largest hospital systems. The graphic above illustrates how the largest “mega-systems” lag other healthcare industry giants, in terms of gross annual revenue.
Amazon and Walmart, retail behemoths that continue to elbow into the healthcare space, posted 2021 revenue that more than quintuples that of the largest health system, Kaiser Permanente. The largest health systems reported increased year-over-year revenue in 2021, largely driven by higher volumes, as elective procedures recovered from the previous year’s dip.
However, according to a recent Kaufman Hall report, while health systems, on average, grew topline revenue by 15 percent year-over-year, they face rising expenses, and have yet to return to pre-pandemic operating margins.
Meanwhile, the larger companies depicted above, including Walmart, Amazon, CVS Health, and UnitedHealth Group, are emerging from the pandemic in a position of financial strength, and continue to double down on vertical integration strategies, configuring an array of healthcare assets into platform businesses focused on delivering value directly to consumers.
A National Bureau of Economic Research working paper found that higher-priced hospitals in competitive markets were associated with lower patient mortality—flying in the face of the common policy narrative that higher-priced care is not higher quality. However, in more concentrated, less-competitive healthcare markets (in which over two-thirds of the nation’s hospitals are located), the study found no correlation between price and quality. Authors of the study analyzed patient outcomes from more than 200K admissions among commercially insured patients, transported by ambulance to about 1,800 hospitals between 2007 and 2014.
The Gist: As hospitals have consolidated, prices have risen by about 30 percent between 2015 to 2019, leading policy experts and regulators to search for ways to rein in price inflation.
While there continues to be widespread consensus that industry consolidation has resulted in unsustainable cost growth, the new study’s findings bring a bit of welcome nuance around impact on quality and outcomes to an otherwise one-sided, price-centric policy narrative.
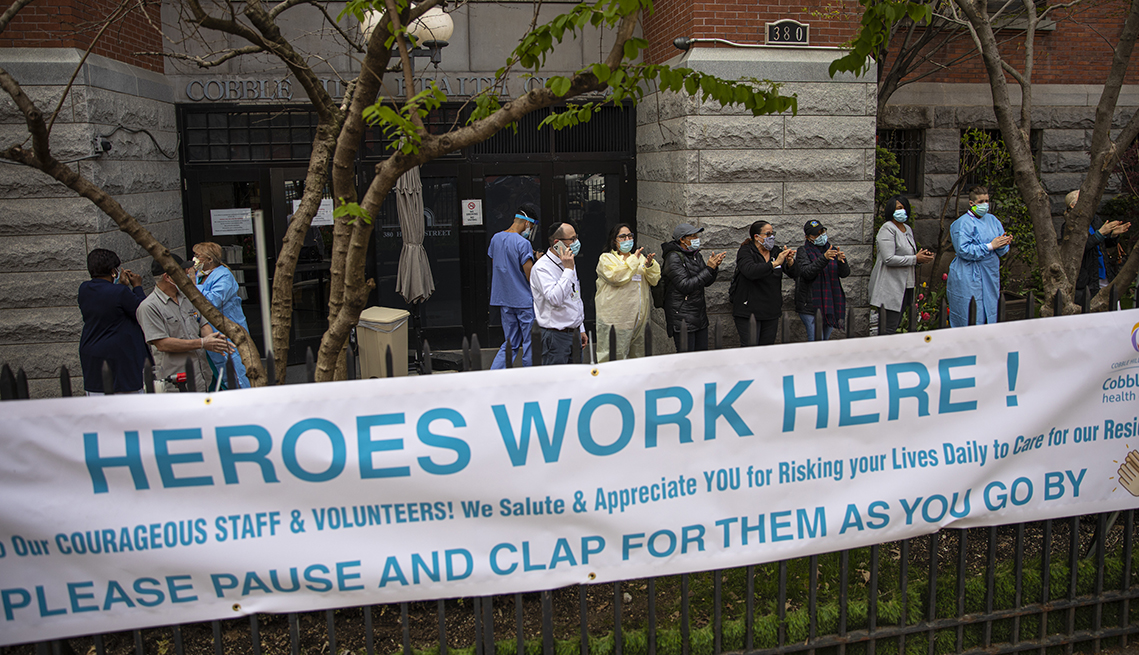
The US healthcare sector added 64K jobs in February, an increase from recent months, but the gains were concentrated in provider offices and home health companies. Hospitals and nursing facilities, which have both struggled with widespread staffing shortages, saw more anemic job growth. In particular, nursing homes have lost 15 percent of their workforce, remaining significantly understaffed even though resident occupancy rates still lag pre-pandemic levels. This week, nursing home groups pushed back against President Biden’s call for minimum staffing levels, calling them unrealistic without federal funding.
The Gist: Hospital and nursing facility workers have taken on some of the most taxing and dangerous jobs during the pandemic, caring for the sickest patients while personally risking COVID infection.
Healthcare workers are increasingly opting for safer, less intense jobs in outpatient care settings like physician offices, or are exiting direct patient care entirely. Even as the pandemic subsides, recruitment and retention of nurses and other caregivers will be of paramount importance, given rising vacancy rates and unabating staff shortages.