Dive Brief:
- CMS is axing its proposed Medicaid Fiscal Accountability Rule, agency head Seema Verma announced via Twitter late Monday afternoon, in a move quickly cheered by provider organizations.
- The rule proposed last year would have increased federal oversight of how states fund their Medicaid programs and potentially resulted in funding cuts for the cash-strapped safety net insurance. Myriad providers, patient advocacy groups and lawmakers in both states and the halls of Congress opposed the rule as a result.
- “We’ve listened closely to concerns that have been raised by our state and provider partners about potential unintended consequences of the proposed rule, which require further study. Therefore, CMS is withdrawing the rule from the regulatory agenda,” Verma said.
Dive Insight:
MFAR was designed to increase fiscal transparency in the 55-year-old Medicaid program, but was quickly met with a firestorm of controversy, with even bipartisan House and Senate members raising concerns it could lead to states being forced to choose between program cuts or raising taxes to replace the lost funding.
One estimate, conducted by Manatt Health for the American Hospital Association, estimated the changes proposed in the rule would cut Medicaid funding by almost $50 billion annually, shrinking the program by 8%.
“Hospitals and health systems will be greatly relieved when the proposed rule is formally withdrawn,” AHA EVP Tom Nickels said in a statement.
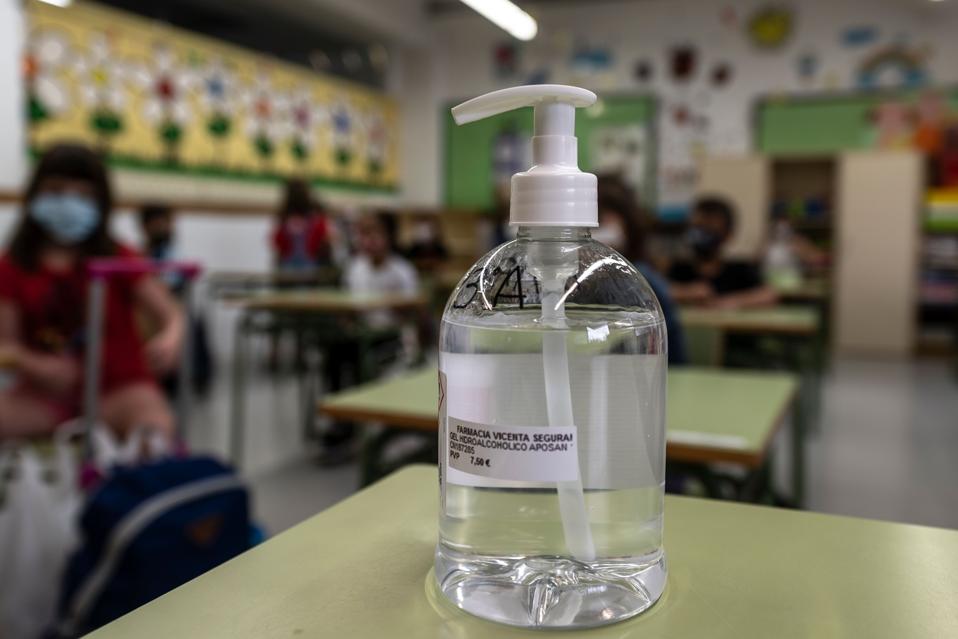
Bruce Siegel, CEO of America’s Essential Hospitals, a lobby representing hospitals serving a disproportionate amount of vulnerable patients, called CMS’ decision “wise and welcome … especially as state budgets and providers strain under the heavy financial burden and economic fallout of COVID-19.”
Medicaid is jointly funded by the states and the federal government. Generally, CMS matches every dollar states spend at rates that vary depending on the state, its covered services and its population. There are no limits for how much federal funding a state can receive, and snowballing spending in Medicaid has resulted in concerns about cost control.
Medicaid spending swelled from $456 billion in 2013 to $576 billion in 2016, per CMS data, mostly due to an expanding federal share.
The most acute worries on the federal side stemmed from supplemental payments, or payments state Medicaid agencies give to providers for going above and beyond routine care, normally for high-need patients or those in underserved areas.
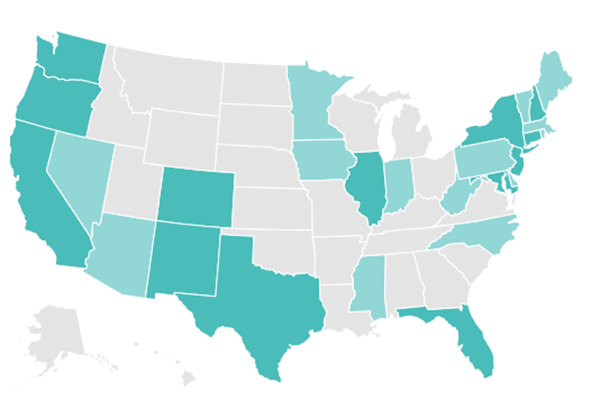
Supplemental payments to healthcare providers have increased from 9.4% of all other payments in 2010 to 17.5% in 2017, according to CMS, and are generally uneven across state lines, contributing to geographic funding disparities.
Oversight agencies, including the Government Accountability Office and the Office of the Inspector General, flagged the growth in payments and called for stronger Medicaid oversight in a series of reports from 2006 to 2015.
As a result, CMS proposed the MFAR rule in November 2019. If finalized, it would require states to report Medicaid payment and financing data at the individual provider level, instead of an aggregate, and establish definitions for “base” and “supplemental” payments. It would also have allowed CMS to sunset existing supplemental payment methodologies after up to three years, requiring states to get approval for a longer period, and close financing loopholes that might allow states to re-use federal Medicaid dollars to fund additional payments.
At the outset, CMS attempted to stamp out criticisms the rule could winnow Medicaid funding. “Alarmist estimates that this rule, if finalized, will suddenly remove billions of dollars from the program and threaten beneficiary access are overblown and without credibility,” Verma wrote in a blog post on the proposal in February.
But the rule received more than 4,000 public comments, most of them negative. The swirling concerns about unintended consequences, especially as COVID-19 exacerbates worries about care access, have now brought CMS back to the drawing board on Medicaid fiscal accountability.
As of late Monday, MFAR remained on the Federal Register.
Other actions from the Trump administration to overhaul Medicaid have faced similar backlash, including unpopular efforts to instill requirements linking coverage to work hours and an early 2020 push to cap federal funding for states in exchange for wider latitude in program administration.