The uncertainty and isolation of the pandemic has taken a heavy toll on mental health.Over a third of adults are currently experiencing anxiety or depression—more than three times as many as early last year. And with access to behavioral health services already challenged before the pandemic, many patients have been turning to telemedicine for support.
Health insurer Cigna found that while use of virtual care for both non-behavioral and behavioral healthcare services peaked in spring 2020, consumers have continued to use telemedicine for mental health needs, while demand for other virtual services tapered off. As of December, about 70 percent of behavioral health claims were for care rendered virtually, compared to just 20 percent across all other services.
The recent surge in demand for virtual mental health services has spurred an influx of investment into digital solutions. A recent Rock Health analysis found investments in the space have more than tripled since 2015. The injection of funds extends to both “generalist” companies (focused on a wide range of virtual services, including behavioral health) and “specialist” companies (focused solely on virtual behavioral health solutions).
Virtual behavioral health not only provides much needed access to care, but patients also prefer the privacy and ready access offered by telemedicine. Moving forward, telemedicine may become the preferred alternative for patients seeking support for mental health needs.
Now that we’ve entered a new phase of the vaccine rollout, with supply beginning to outstrip demand and all adults eligible to get vaccinated, we’re hearing from a number of health systems that their strategy is shifting from a centralized, scheduled approach to a more distributed, access-driven model. They’re recognizing that, in order to get the vaccine to harder-to-reach populations, and to convince reticent individuals to get vaccinated, they’ll need to lean more heavily on walk-in clinics, community settings, and yes—primary care physicians.
For some time, the primary care community has been complaining they’ve been overlooked in the national vaccination strategy, with health systems, pharmacy chains, and mass vaccination sites getting the lion’s share of doses. But now that we’re moving beyond the “if you build it, they will come” phase, and into the “please come get a shot” phase, we’ll need to lean much more heavily on primary care doctors, and the trusted relationships they have with their patients.
As one chief clinical officer told us this week, that means not just solving the logistical challenges of distributing vaccines to physician offices (which would be greatly aided by single-dose vials of vaccine, among other things), but planning for patient outreach. Simply advertising vaccine availability won’t suffice—now the playbook will have to include reaching out to patients to encourage them to sign up.
There will be workflow challenges as well, particularly while we await those single-dose shots—primary care clinics will likely need to schedule blocks of appointments, setting aside specific times of day or days of the week for vaccinations. The more distributed the vaccine rollout, the more operationally complex it will become. Health systems won’t be able to “get out of the vaccine business”, as one health system executive told us, because many have spent the past decade or more buying up primary care practices and rolling out urgent care locations. Now those assets must be enlisted in the service of vaccination rollout.
Health systems will have to orchestrate a “pull” strategy for vaccines, rather than the vaccination “push” they’ve been conducting for the past several months. To put it in military terms,the vaccination “air war” is over—now it’s time for what’s likely to be a protracted and difficult “ground campaign”.
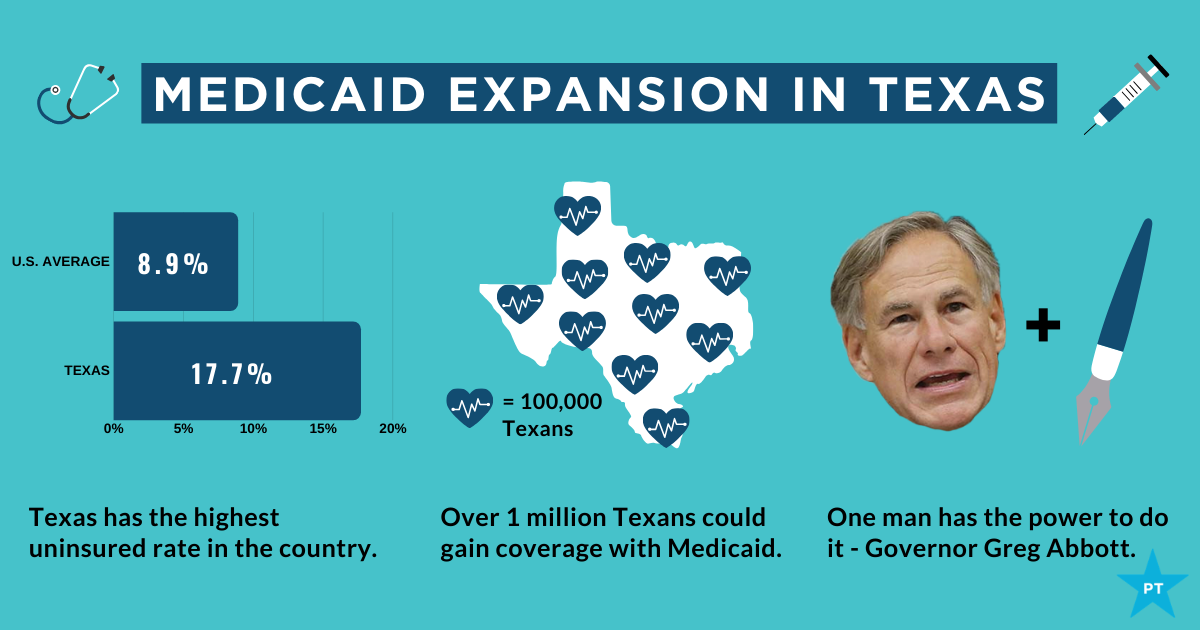
The showdown between the Biden administration and the state of Texas over Medicaid expansion continued to escalate this week. Sen. John Cornyn (R-TX) said he planned to place a hold on the confirmation of Chiquita Brooks-LaSure to become Administrator of the Centers for Medicare & Medicaid Services (CMS), until his concerns over the agency’s move last week to rescind a waiver extension previously granted by the Trump administration were addressed.
The so-called “1115 waiver”—worth more than $11B annually—would have extended by a decade Texas’ ability to use Medicaid funds to cover hospital costs for uninsured residents, rather than expanding Medicaid coverage under the Affordable Care Act (ACA). In rescinding the waiver extension, the Biden administration cited the lack of a public notice process before the waiver was granted, and said that the state’s existing waiver would instead expire next year, as previously scheduled.
Sources inside the administration told the Washington Post last week thatthe move was intended to force Texas’ hand on Medicaid expansion; the state is one of 12 that have not expanded Medicaid, leaving it with the largest share of uninsured residents of any state, with eligibility currently limited to pregnant women, children, people with disabilities, and families with monthly incomes under $300 per month, or 13.6 percent of the federal poverty level.
Enticing the dozen remaining holdout states to expand Medicaid is an important policy priority for the new administration.A key component of the recently passed American Rescue Plan Act is a package of enhanced incentives for those states to expand eligibility, offering an extended 90 percent federal match, in addition to increased funding for existing Medicaid populations.
Although none of the non-expansion states have budged yet, there has been renewed focus among state lawmakers on Medicaid expansion, including in Texas, where the idea had garnered bipartisan support. However, on Thursday, the Texas legislature voted down a proposal aimed at pushing the state toward expanding coverage for the uninsured, by an 80-68 margin. Meanwhile, the rescission of Texas’ waiver has angered the state’s Republican leadership, along with the Texas Hospital Association, whose members have benefited from the waiver’s use of funds to reimburse them for delivering uncompensated care.
While Cornyn’s hold will not ultimately stop the confirmation of the new CMS leader, the escalation on both sides over the past several days surely makes finding a compromise solution less likely. The Biden health policy team is said to be developing a new proposal, as part of an upcoming legislative package, to use the ACA marketplace to offer coverage to people in non-expansion states who might otherwise be eligible for Medicaid—yet another attempt to address one of the longest-standing points of contention stemming from the 2010 health reform law.
Of 26 health systems surveyed by MedCity News, nearly half used automated tools to respond to the Covid-19 pandemic, but none of them were regulated. Even as some hospitals continued using these algorithms, experts cautioned against their use in high-stakes decisions.
A year ago, Michigan Medicine faced a dire situation. In March of 2020, the health system predicted it would have three times as many patients as its 1,000-bed capacity — and that was the best-case scenario. Hospital leadership prepared for this grim prediction by opening a field hospital in a nearby indoor track facility, where patients could go if they were stable, but still needed hospital care. But they faced another predicament: How would they decide who to send there?
Two weeks before the field hospital was set to open, Michigan Medicine decided to use a risk model developed by Epic Systems to flag patients at risk of deterioration. Patients were given a score of 0 to 100, intended to help care teams determine if they might need an ICU bed in the near future. Although the model wasn’t developed specifically for Covid-19 patients, it was the best option available at the time, said Dr. Karandeep Singh, an assistant professor of learning health sciences at the University of Michigan and chair of Michigan Medicine’s clinical intelligence committee. But there was no peer-reviewed research to show how well it actually worked.
Researchers tested it on over 300 Covid-19 patients between March and May. They were looking for scores that would indicate when patients would need to go to the ICU, and if there was a point where patients almost certainly wouldn’t need intensive care.
“We did find a threshold where if you remained below that threshold, 90% of patients wouldn’t need to go to the ICU,” Singh said. “Is that enough to make a decision on? We didn’t think so.”
But if the number of patients were to far exceed the health system’s capacity, it would be helpful to have some way to assist with those decisions.
“It was something that we definitely thought about implementing if that day were to come,” he said in a February interview.
Thankfully, that day never came.
The survey Michigan Medicine is one of 80 hospitals contacted by MedCity News between January and April in a survey of decision-support systems implemented during the pandemic. Of the 26 respondents, 12 used machine learning tools or automated decision systems as part of their pandemic response. Larger hospitals and academic medical centers used them more frequently.
Faced with scarcities in testing, masks, hospital beds and vaccines, several of the hospitals turned to models as they prepared for difficult decisions. The deterioration index created by Epic was one of the most widely implemented — more than 100 hospitals are currently using it — but in many cases, hospitals also formulated their own algorithms.
They built models to predict which patients were most likely to test positive when shortages of swabs and reagents backlogged tests early in the pandemic. Others developed risk-scoring tools to help determine who should be contacted first for monoclonal antibody treatment, or which Covid patients should be enrolled in at-home monitoring programs.
MedCity News also interviewed hospitals on their processes for evaluating software tools to ensure they are accurate and unbiased. Currently, the FDA does not require some clinical decision-support systems to be cleared as medical devices, leaving the developers of these tools and the hospitals that implement them responsible for vetting them.
Among the hospitals that published efficacy data, some of the models were only evaluated through retrospective studies. This can pose a challenge in figuring out how clinicians actually use them in practice, and how well they work in real time. And while some of the hospitals tested whether the models were accurate across different groups of patients — such as people of a certain race, gender or location — this practice wasn’t universal.
As more companies spin up these models, researchers cautioned that they need to be designed and implemented carefully, to ensure they don’t yield biased results.
An ongoing review of more than 200 Covid-19 risk-prediction models found that the majority had a high risk of bias, meaning the data they were trained on might not represent the real world.
“It’s that very careful and non-trivial process of defining exactly what we want the algorithm to be doing,” said Ziad Obermeyer, an associate professor of health policy and management at UC Berkeley who studies machine learning in healthcare. “I think an optimistic view is that the pandemic functions as a wakeup call for us to be a lot more careful in all of the ways we’ve talked about with how we build algorithms, how we evaluate them, and what we want them to do.”
Algorithms can’t be a proxy for tough decisions Concerns about bias are not new to healthcare. In a paper published two years ago, Obermeyer found a tool used by several hospitals to prioritize high-risk patients for additional care resources was biased against Black patients. By equating patients’ health needs with the cost of care, the developers built an algorithm that yielded discriminatory results.
More recently, a rule-based system developed by Stanford Medicine to determine who would get the Covid-19 vaccine first ended up prioritizing administrators and doctors who were seeing patients remotely, leaving out most of its 1,300 residents who had been working on the front lines. After an uproar, the university attributed the errors to a “complex algorithm,” though there was no machine learning involved.
Both examples highlight the importance of thinking through what exactly a model is designed to do — and not using them as a proxy to avoid the hard questions.
“The Stanford thing was another example of, we wanted the algorithm to do A, but we told it to do B. I think many health systems are doing something similar,” Obermeyer said. “You want to give the vaccine first to people who need it the most — how do we measure that?”
The urgency that the pandemic created was a complicating factor. With little information and few proven systems to work with in the beginning, health systems began throwing ideas at the wall to see what works. One expert questioned whether people might be abdicating some responsibility to these tools.
“Hard decisions are being made at hospitals all the time, especially in this space, but I’m worried about algorithms being the idea of where the responsibility gets shifted,” said Varoon Mathur, a technology fellow at NYU’s AI Now Institute, in a Zoom interview. “Tough decisions are going to be made, I don’t think there are any doubts about that. But what are those tough decisions? We don’t actually name what constraints we’re hitting up against.”
The wild, wild west There currently is no gold standard for how hospitals should implement machine learning tools, and little regulatory oversight for models designed to support physicians’ decisions, resulting in an environment that Mathur described as the “wild, wild west.”
How these systems were used varied significantly from hospital to hospital.
Early in the pandemic, Cleveland Clinic used a model to predict which patients were most likely to test positive for the virus as tests were limited. Researchers developed it using health record data from more than 11,000 patients in Ohio and Florida, including 818 who tested positive for Covid-19. Later, they created a similar risk calculator to determine which patients were most likely to be hospitalized for Covid-19, which was used to prioritize which patients would be contacted daily as part of an at-home monitoring program.
Initially, anyone who tested positive for Covid-19 could enroll in this program, but as cases began to tick up, “you could see how quickly the nurses and care managers who were running this program were overwhelmed,” said Dr. Lara Jehi, Chief Research Information Officer at Cleveland Clinic. “When you had thousands of patients who tested positive, how could you contact all of them?”
While the tool included dozens of factors, such as a patient’s age, sex, BMI, zip code, and whether they smoked or got their flu shot, it’s also worth noting that demographic information significantly changed the results. For example, a patient’s race “far outweighs” any medical comorbidity when used by the tool to estimate hospitalization risk, according to a paper published in Plos One. Cleveland Clinic recently made the model available to other health systems.
Others, like Stanford Health Care and 731-bed Santa Clara County Medical Center, started using Epic’s clinical deterioration index before developing their own Covid-specific risk models. At one point, Stanford developed its own risk-scoring tool, which was built using past data from other patients who had similar respiratory diseases, such as the flu, pneumonia, or acute respiratory distress syndrome. It was designed to predict which patients would need ventilation within two days, and someone’s risk of dying from the disease at the time of admission.
Stanford tested the model to see how it worked on retrospective data from 159 patients that were hospitalized with Covid-19, and cross-validated it with Salt Lake City-based Intermountain Healthcare, a process that took several months. Although this gave some additional assurance — Salt Lake City and Palo Alto have very different populations, smoking rates and demographics — it still wasn’t representative of some patient groups across the U.S.
“Ideally, what we would want to do is run the model specifically on different populations, like on African Americans or Hispanics and see how it performs to ensure it’s performing the same for different groups,” Tina Hernandez-Boussard, an associate professor of medicine, biomedical data science and surgery at Stanford, said in a February interview. “That’s something we’re actively seeking. Our numbers are still a little low to do that right now.”
Stanford planned to implement the model earlier this year, but ultimately tabled it as Covid-19 cases fell.
‘The target is moving so rapidly’ Although large medical centers were more likely to have implemented automated systems, there were a few notable holdouts. For example, UC San Francisco Health, Duke Health and Dignity Health all said they opted not to use risk-prediction models or other machine learning tools in their pandemic responses.
“It’s pretty wild out there and I’ll be honest with you — the dynamics are changing so rapidly,” said Dr. Erich Huang, chief officer for data quality at Duke Health and director of Duke Forge. “You might have a model that makes sense for the conditions of last month but do they make sense for the conditions of next month?”
That’s especially true as new variants spread across the U.S., and more adults are vaccinated, changing the nature and pace of the disease. But other, less obvious factors might also affect the data. For instance, Huang pointed to big differences in social mobility across the state of North Carolina, and whether people complied with local restrictions. Differing social and demographic factors across communities, such as where people work and whether they have health insurance, can also affect how a model performs.
“There are so many different axes of variability, I’d feel hard pressed to be comfortable using machine learning or AI at this point in time,” he said. “We need to be careful and understand the stakes of what we’re doing, especially in healthcare.”
Leadership at one of the largest public hospitals in the U.S., 600-bed LAC+USC Medical Center in Los Angeles, also steered away from using predictive models, even as it faced an alarming surge in cases over the winter months.
At most, the hospital used alerts to remind physicians to wear protective equipment when a patient has tested positive for Covid-19.
“My impression is that the industry is not anywhere near ready to deploy fully automated stuff just because of the risks involved,” said Dr. Phillip Gruber, LAC+USC’s chief medical information officer. “Our institution and a lot of institutions in our region are still focused on core competencies. We have to be good stewards of taxpayer dollars.”
When the data itself is biased Developers have to contend with the fact that any model developed in healthcare will be biased, because the data itself is biased; how people access and interact with health systems in the U.S. is fundamentally unequal.
How that information is recorded in electronic health record systems (EHR) can also be a source of bias, NYU’s Mathur said. People don’t always self-report their race or ethnicity in a way that fits neatly within the parameters of an EHR. Not everyone trusts health systems, and many people struggle to even access care in the first place.
“Demographic variables are not going to be sharply nuanced. Even if they are… in my opinion, they’re not clean enough or good enough to be nuanced into a model,” Mathur said.
The information hospitals have had to work with during the pandemic is particularly messy. Differences in testing access and missing demographic data also affect how resources are distributed and other responses to the pandemic.
“It’s very striking because everything we know about the pandemic is viewed through the lens of number of cases or number of deaths,” UC Berkeley’s Obermeyer said. “But all of that depends on access to testing.”
At the hospital level, internal data wouldn’t be enough to truly follow whether an algorithm to predict adverse events from Covid-19 was actually working. Developers would have to look at social security data on mortality, or whether the patient went to another hospital, to track down what happened.
“What about the people a physician sends home — if they die and don’t come back?” he said.
Researchers at Mount Sinai Health System tested a machine learning tool to predict critical events in Covid-19 patients — such as dialysis, intubation or ICU admission — to ensure it worked across different patient demographics. But they still ran into their own limitations, even though the New York-based hospital system serves a diverse group of patients.
They tested how the model performed across Mount Sinai’s different hospitals. In some cases, when the model wasn’t very robust, it yielded different results, said Benjamin Glicksberg, an assistant professor of genetics and genomic sciences at Mount Sinai and a member of its Hasso Plattner Institute for Digital Health.
They also tested how it worked in different subgroups of patients to ensure it didn’t perform disproportionately better for patients from one demographic.
“If there’s a bias in the data going in, there’s almost certainly going to be a bias in the data coming out of it,” he said in a Zoom interview. “Unfortunately, I think it’s going to be a matter of having more information that can approximate these external factors that may drive these discrepancies. A lot of that is social determinants of health, which are not captured well in the EHR. That’s going to be critical for how we assess model fairness.”
Even after checking for whether a model yields fair and accurate results, the work isn’t done yet. Hospitals must continue to validate continuously to ensure they’re still working as intended — especially in a situation as fast-moving as a pandemic.
A bigger role for regulators All of this is stirring up a broader discussion about how much of a role regulators should have in how decision-support systems are implemented.
Of the hospitals surveyed by MedCity News, none of the models they developed had been cleared by the FDA, and most of the external tools they implemented also hadn’t gone through any regulatory review.
“My experience suggests that most models are put into practice with very little evidence of their effects on outcomes because they are presumed to work, or at least to be more efficient than other decision-making processes,” Kellie Owens, a researcher for Data & Society, a nonprofit that studies the social implications of technology, wrote in an email. “I think we still need to develop better ways to conduct algorithmic risk assessments in medicine. I’d like to see the FDA take a much larger role in regulating AI and machine learning models before their implementation.”
Developers should also ask themselves if the communities they’re serving have a say in how the system is built, or whether it is needed in the first place. The majority of hospitals surveyed did not share with patients if a model was used in their care or involve patients in the development process.
In some cases, the best option might be the simplest one: don’t build.
In the meantime, hospitals are left to sift through existing published data, preprints and vendor promises to decide on the best option. To date, Michigan Medicine’s paper is still the only one that has been published on Epic’s Deterioration Index.
Care teams there used Epic’s score as a support tool for its rapid response teams to check in on patients. But the health system was also looking at other options.
“The short game was that we had to go with the score we had,” Singh said. “The longer game was, Epic’s deterioration index is proprietary. That raises questions about what is in it.”
As health systems look to address the “social determinants of health”, one obvious but often overlooked place to start is with their own employees. The left side of the graphic below shows forecasted employment growth and salaries across a range of healthcare occupations. Many of the fastest-growing healthcare jobs—including home health and personal aides, medical assistants, and phlebotomists—are among the lowest-paid.
Case in point: home health and personal care aides are among the top 20 fastest-growing occupations in the US, and median wage for these jobs is only about $12 per hour, or around 200 percent of the federal poverty level—well below the living wage in many parts of the nation. (Note that this analysis does not include support staff who are not healthcare specific, like custodial or dietary workers, so the number of low-wage workers at health systems is likely higher.)
Among of the many struggles lower-income healthcare employees face is finding affordable housing. Using fair market rent data from the US Department of Housing and Urban Development, the right side of the graphic shows that healthcare support workers, even at the 90th percentile salary level, struggle to afford rent in the majority of the 50 largest US metros areas. In particular, home health aides in the top decile of earners can only afford rent in 14 percent of major cities.
These disparities have caught the attention of lawmakers. The $400B in President Biden’s proposed infrastructure plan devoted to home healthcare for seniors includes tactics to increase the wages and quality of life for these caregivers. But as we await policy solutions, health systems should pay careful attention to issues of housing insecurity and other structural challenges facing their workers and look to increase wages and provide targeted support to these critical team members.
In a vote of 384-38, the House on Tuesday passed a bill that eliminates the 2% cut to Medicare payments until the end of 2021. However, the bill proposes to offset the change by increasing the sequester cuts in 2030.
WHY THIS MATTERS
The cuts were triggered by a federal budget sequestration.
Hospitals, physicians and other providers protested the 2% cuts as coming at a time when they were struggling financially and clinically to handle the COVID-19 pandemic.
The bill also makes several technical changes to the rural health clinic provisions that were included in the Consolidated Appropriations Act. Specifically, the CAA required that the payment rate for RHCs, including provider-based RHCs certified after Dec. 31, 2019, to be capped at $100 per visit, starting from April 1, 2021.
This rate will increase over time based on the Medicare Economic Index, but will remain well below typical provider-based RHC rates. The bill would correct the Dec. 31, 2019, date to Dec. 31, 2020, and include both Medicare-enrolled RHCs located in a hospital with less than 50 beds and RHCs that have submitted an application for Medicare enrollment as of this date, according to the AHA.
THE LARGER TREND
Last year, Congress paused the 2% Medicare cuts, but they were to resume on April 1.
The Centers for Medicare and Medicaid Services instructed Medicare administrative contractors to hold all claims with dates of service on or after April 1 for a short period until potential legislation was enacted.
In March, the House passed the bill to delay the cuts, and the Senate approved it later that month, but with an amendment to delay through December 31 and ensure that the cost of the delay is paid for.
PROVIDER REACTION
Providers have reacted positively to the news.
American Hospital Association president and CEO Rick Pollack said, “Even though our country is making great progress by vaccinating millions of people a day, it is clear that this pandemic is far from over and that there is an urgent need to keep hospitals, health systems and our heroic caregivers strong.”
American Medical Association president Dr. Susan R. Bailey said, “The Senate and House, Democrats and Republicans, have overwhelmingly acknowledged that cutting Medicare payments during a pandemic is ill-conceived policy. Physician practices are already distressed, and arbitrary 2% across-the-board Medicare cuts would have been devastating.”
America’s Essential Hospitals SVP of policy and advocacy Beth Feldpush said, “Extending the moratorium through the end of this year provides much-needed relief for essential hospitals, which continue to face heavy financial pressure from their frontline response to COVID-19. The sequester would weaken the ability of our hospitals to care for the communities of color that have suffered disproportionately from the pandemic.”
In early 2013, Hoag Memorial Hospital Presbyterian in Orange County, California, joined with St. Joseph Health, a local Catholic hospital chain, amid enthusiastic promises that their affiliation would broaden access to care and improve the health of residents across the community.
Eight years later, Hoag says this vision of achieving “population health” is dead, and it wants out. It is embroiled in a legal battle for independence from Providence, a Catholic health system with 51 hospitals across seven states, which absorbed St. Joseph in 2016, bringing Hoag along with it.
In a lawsuit filed in Orange County Superior Court last May, Hoag argues that remaining a “captive affiliate” of the nation’s 10th-largest health system, headquartered nearly 1,200 miles away in Washington state, constrains its ability to meet the needs of the local population.
Hoag doctors say that Providence’s drive to standardize treatment decisions across its chain — largely through a shared Epic electronic records system — often conflicts with their own judgment of best medical practices. And they recoil against restrictions on reproductive care they say Providence illegally imposes on them through its adherence to the Catholic health directives established by the United States Conference of Catholic Bishops.
“Their large widespread system is very different than the laser focus Hoag has on taking care of its community,” said Hoag CEO Robert Braithwaite. “When Hoag needed speed and agility, we got inadequate responses or policies that were just wrong for us. We found ourselves frustrated with a big health system that had a generic approach to health care.”
Providence insists it wants to stay with Hoag, a financial powerhouse — even as the two sides engage in secret settlement talks that could end the marriage.
“We believe we are better together,” said Erik Wexler, president of Providence South, which includes the group’s operations in California, Texas and New Mexico. “The best way to do that is to collaborate.” He cited joint investments in Hoag Orthopedic Institute and in Be Well OC, a kind of mental health collaborative, as fruits of the affiliation.
“If we are separate,” Wexler added, “there is a chance we may begin to cannibalize each other and drive the cost of care up.”
Research over the past several years, however, has shown that it is the consolidation of hospitals into fewer and larger groups, with greater bargaining clout, that tends to raise medical prices — often with little improvement in the quality of care.
“Mergers are a self-centered pursuit of stability by hospitals and hospital systems that hope to get so big that they can survive the anarchy of U.S. health care,” said Alan Sager, a professor at Boston University’s School of Public Health.
Wexler argued that price increases linked to consolidation are less of a worry in Orange County, geographically small but densely populated with 3.2 million residents and 28 acute care hospitals. Given the proximity of so many hospitals, Wexler said, counterproductive duplication of medical services is more of a concern.
Unlike many local community hospitals that seek larger partners to survive, Hoag, one of Orange County’s premier medical institutions, is financially robust and perfectly able to stand on its own. It has the advantage of operating in one of Orange County’s most affluent areas, with two acute care hospitals and an orthopedic specialty hospital in Newport Beach and Irvine. It is the beneficiary of numerous wealthy donors, including bond market billionaire Bill Gross and thriller novelist Dean Koontz.
In 2020, Hoag’s net assets, essentially its net worth, stood at about $3.3 billion — nearly 20% of the total for all Providence-affiliated facilities, even though Hoag has only three of the group’s 51 hospitals. Hoag generated operating income of $38 million last year, while Providence posted a $306 million operating loss.
But Providence is hardly a financial weakling. It is sitting on a mountain of unrestricted cash and investments worth $15.3 billion as of Dec. 31. And despite its hefty reserves, it received $1.1 billion in coronavirus relief grants last year under the federal CARES Act, and millions more from the Federal Emergency Management Agency.
Providence does not own Hoag, since no money changed hands and their assets were not commingled. But Providence is able to keep Hoag from walking away because it has a majority on the governing body that was set up to oversee the original affiliation with St. Joseph.
Hoag executives also express frustration at what they describe as efforts by Providence to interfere with their financial, labor and supply decisions.
Providence, in turn, worries that “if Hoag disaffiliates with Providence, it has the potential to impact our credit rating,”Wexler said.
Despite its insistence on the value of the affiliation, Providence officials are said to be willing to end the affiliation in exchange for payment of an undisclosed amount that Hoag considers unwarranted. Wexler and Hoag executives declined to comment on their discussions. A trial start date has not been set, but on April 26 the court will hear a motion from Hoag to expedite it.
While its financial fortitude distinguishes it from many other community hospitals tied to larger partners, Hoag’s experience with Providence is hardly uncommon amid widespread consolidation in the hospital industry and the growing influence of Catholic health care in the U.S.
“The bigger your parent organization becomes, the smaller your voice is within the system, and that’s part of what Hoag has been complaining about,” said Lois Uttley, director of the women’s health program at Community Catalyst, a Boston-based patient advocacy group that monitors hospital mergers.
“Compounding the problem is the fact that the system in this case is Catholic-run, because then, in addition to having an out-of-town system headquarters calling the shots, you also have to contend with governance from Catholic bishops,” Uttley said. “So you have two bosses, in a sense.”
Hoag is not the only hospital seeking to flee this dynamic. Last year, for example, Virginia Mason Memorial hospital in Yakima, Washington, said it would separate from its parent, Seattle-based Virginia Mason Health System, to avoid a pending merger with CHI Franciscan, part of the Catholic hospital giant CommonSpirit Health.
Mergers and acquisitions have led to the increasing dominance of mega hospital chains in U.S. health care over the past several years. From 2013 to 2018, the revenue of the 10 largest health systems grew 82%, compared with 45% for all other hospital groups, according to a recent study by Deloitte, the consulting and auditing firm.
Researchers expect the trend to accelerate as large health systems swallow smaller facilities economically weakened by the pandemic, and a growing trend toward outpatient care reduces demand for hospital beds.
Four of the 10 largest U.S. hospital systems are Catholic, including Chicago-based CommonSpirit Health, St. Louis-based Ascension, Livonia, Michigan-based Trinity Health and Providence. A study by Community Catalyst found that 1 in 6 acute care hospital beds are in Catholic facilities, and that 52 hospitals operating under Catholic restrictions were the sole acute care facilities in their regions last year, up from 30 in 2013.
“We need to make this a national conversation,” said Dr. Jeffrey Illeck, a Hoag OB-GYN.
He was among a group of Hoag OB-GYNs who signed a letter to then-California Attorney General Xavier Becerra in October, alleging that Providence frequently declined to authorize contraceptive treatments, such as intrauterine devices and tubal ligations — in breach of the conditions imposed by Becerra’s predecessor, Kamala Harris, when she approved the original affiliation with St. Joseph in 2013.
Wexler said he is confident the attorney general’s probe will provide “clarity that Providence has done nothing wrong.”
A particularly bitter disagreement between the two sides concerns a rupture last year within St. Joseph Heritage Healthcare, a physician group belonging to Providence that included both St. Joseph and Hoag doctors. In November, the group notified thousands of patients that their Hoag specialists were no longer part of the network and that they needed to choose new doctors.
Wexler said that was the inevitable result of a decision by the Hoag physicians to negotiate separate HMO contracts, an assertion Braithwaite contested. The move disrupted patient care just as the winter covid surge was gaining momentum, he said.
Perhaps the biggest frustration for most Hoag administrators and physicians is Providence’s desire to standardize care across all 51 hospitals through their shared Epic electronic records system.
Hoag doctors say Providence controls the contents of the Epic system and that the care protocols in it, often driven by cost considerations, frequently collide with their own clinical decisions. Any changes must be debated among all the hospitals in the system and adopted by consensus — a laborious undertaking.
Dr. Richard Haskell, a cardiologist at Hoag, recalled a dispute over intravenous Tylenol, which Hoag’s orthopedists prefer because they say it works well and furthered a concerted effort to reduce opioid addiction. Providence took IV Tylenol off its list of accepted drugs, and the Hoag orthopedists “were very upset,” Haskell said.
They eventually got it back on that list, but with the condition that they could order it only one dose at a time. That meant nurses had to call the doctor every four hours for a new order. “Doctors probably felt, ‘Screw it, I don’t want to get woken up every four hours,’ so they probably just gave them narcotics,’” Haskell said.
He said that before agreeing to adopt Providence’s Epic system, Hoag had received written assurances it could make changes that included its preferred treatment choices for various conditions. But it quickly became clear that was not going to happen, he said.
“We couldn’t make any changes at all, so we were stuck with their system,” Haskell said. “I don’t want to be in a system bogged down by bureaucracy that requires 51 hospitals to vote on it.”
Wexler said Hoag understood exactly what it had signed up for. “They knew full well that there would be a collaborative approach across all of Providence, including Hoag, to make decisions on what standardizations would happen across the entire system,” he said. “It is not easy if one hospital wants to create its own specific pathway.”
Despite Hoag’s concerns about lesser standards of care, Braithwaite could not cite an example of an adverse outcome that had resulted from it. And Hoag’s strong reputation seems untarnished, as reflected in the high rankings and awards it continues to garner — and tout on its website.
Still, the affiliation’s days seem numbered. Hoag is no longer on the Providence website or in its marketing materials, and in many cases — such as the St. Joseph Heritage schism — the two groups are already going their separate ways.
“They are certainly acting like we are competitors, and I assume that means they know the disaffiliation is imminent,” Braithwaite said.
Wexler, while reiterating that Providence wants to maintain the current arrangement, was nonetheless able to imagine a different outcome: “What we would do post-affiliation,” he said, “is to continue to look for opportunities to collaborate.”
Although urgent care centers deter some lower-acuity patients from a costly emergency department visit, they are not associated with a drop in total healthcare spending, according to a study published in Health Affairsin April.
For the study, researchers used insurance claims and enrollment data from 2008 to 2019 from a managed care plan to understand if the presence of an urgent care center substantially decreased lower-acuity ED visits.
The authors found that the entry of an urgent care center into a ZIP code deterred lower-acuity ED visits, but the effect was small.
The study found that the reduction of just one lower-acuity ED visit was associated with 37 additional urgent care visits. In other words, the number of urgent care visits per enrollee required to reduce one ER visit is 37.
The study authors found that the prevention of each $1,646 lower-acuity ED visit was offset by an increase of $6,237 in urgent care center costs.
As a result, the study authors said that despite ED visits costing more per visit, the use of urgent care centers increased net overall spending on lower-acuity care.
“This study documents for the first time that urgent care centers are associated with increased overall costs for lower-acuity visits across the ED and urgent care settings,” the study authors concluded.
The financial challenges caused by the COVID-19 pandemic forced hundreds of hospitals across the nation to furlough, lay off or reduce pay for workers, and others have had to scale back services or close.
Lower patient volume, canceled elective procedures and higher expenses tied to the pandemic have created a cash crunch for hospitals, and hospitals are taking a number of steps to offset financial damage. Executives, clinicians and other staff are taking pay cuts, capital projects are being put on hold, and some employees are losing their jobs. More than 260 hospitals and health systems furloughed workers in the last year, and dozens of others have implemented layoffs.
Below are nine hospitals and health systems that are laying off employees. Some of the layoffs were attributed to financial strain caused by the pandemic.
1. Boca Raton, Fla.-based Cancer Treatment Centers of America is selling its hospital in Philadelphia and will lay off the facility’s 365 employees, according to a closure notice filed with the state. Cancer Treatment Centers of America said it anticipates the layoffs in Philadelphia will begin after May 30, according to the Philadelphia Business Journal.
2.Providence Queen of the Valley Medical Center in Napa, Calif., will lay off 10 employees, The Napa Valley Register reported April 11. The layoffs will affect six emergency department technicians and four cooks. The COVID-19 pandemic had a “profound effect” on the hospital system, including volume and revenue reductions, a Providence spokesperson told The Napa Valley Register. As a result of volume declines in its ED, the health system is reducing staffing.
3. Olympia Medical Center in Los Angeles closed March 31. The closure resulted in the layoffs of 451 employees.
4. The outgoing owners ofProvidence Behavioral Health Hospital in Holyoke, Mass., are laying off the hospital’s 151 employees, effective April 20, according to MassLive. Trinity Health of New England, part of Livonia, Mich.-based Trinity Health, is selling the hospital to Health Partners New England, which plans to take over the hospital April 20.
6. Plattsburgh, N.Y.-based Champlain Valley Physicians Hospitalplans to cut 60 jobs. The hospital, which is facing a $6.5 million deficit in fiscal year 2021, said the cuts include 10 people who were laid off or had permanent hour reductions, 12 people who are planning retirement, and the rest are open positions that will not be filled, according to a March 9 NBC 5 report.
7. Buffalo, N.Y.-based Catholic Healthannounced March 19 that it plans to end inpatient services and close the intensive care unit at its St. Joseph campus in Cheektowaga, N.Y. The changes will result in some positions being eliminated. Catholic Health said it will try to find affected employees comparable positions within the system.
8. Upper Allegheny Health System, a two-hospital system based in Olean, N.Y., plans to reduce acute care and surgical services at Bradford (Pa.) Regional Medical Center. Under the plan, the acute care and surgical services will be moved to the health system’s other hospital, Olean General Hospital, effective May 1. There will be a minimal number of layoffs resulting from the consolidation of services, a spokesperson told WHYY.
9. Philadelphia-based Tower Health laid off 15 workers at St. Christopher’s Hospital for Children, including four physicians, in March, according to The Philadelphia Inquirer. Tower Health ended the second half of last year with an operating loss of $31 million, according to the report.