Virtual care company Doctor on Demand and clinical navigator Grand Rounds have announced plans to merge, creating a multibillion-dollar digital health firm.
The goal of combining the two venture-backed companies, which will continue to operate under their existing brands for the time being, is to integrate medical and behavioral healthcare with patient navigation and advocacy to try to better coordinate care in the fragmented U.S. medical system.
Financial terms of the deal, which is expected to close in the first half of this year, were not disclosed, but it is an all-stock deal with no capital from outside investors, company spokespeople told Healthcare Dive.
Dive Insight:
The digital health boom stemming from the coronavirus pandemic resulted in a flurry of high-profile deals last year, including the biggest U.S. digital health acquisition of all time: Teladoc Health’s $18.5 billion buy of chronic care management company Livongo. Such tie-ups in the virtual care space come as a slew of growing companies race to build out end-to-end offerings, making them more attractive to potential payer and employer clients and helping them snap up valuable market share.
Ten-year-old Grand Rounds peddles a clinical navigation platform and patient advocacy tools to businesses to help their workers navigate the complex and disjointed healthcare system, while nine-year-old Doctor on Demand is one of the major virtual care providers in the U.S.
Merging is meant to ameliorate the problem of uncoordinated care while accelerating telehealth utilization in previously niche areas like primary care, specialty care, behavioral health and chronic condition management, the two companies said in a Tuesday release.
Grand Rounds and Doctor on Demand first started discussing a potential deal in the early days of the coronavirus pandemic, as both companies saw surging demand for their offerings. COVID-19 completely overhauled how healthcare is delivered as consumers sought safe digital access to doctors, resulting in massive tailwinds for digital health companies and unprecedented investor interest in the sector.
Equity funding in digital health globally hit an all-time high of $26.5 billion in 2020, according to CB Insights, with mental and women’s health services seeing particularly fast growth in investor interest.
Both companies reported strong funding rounds in the middle of last year, catapulting Grand Rounds and Doctor on Demand to enterprise valuations of $1.34 billion and $821 million respectively, according to private equity marketplace SharesPost. Doctor on Demand says its current valuation is $875 million.
The combined entity will operate in an increasingly competitive space against such market giants as Teladoc, which currently sits at a market cap of $31.3 billion, and Amwell, which went public in September last year and has a market cap of $5.1 billion.
Grand Rounds CEO Owen Tripp will serve as CEO of the combined business, while Doctor on Demand’s current CEO Hill Ferguson will continue to lead the Doctor on Demand business as the two companies integrate and will join the combined company’s board.
Walmart has continued to grow its presence in healthcare over the past few years, with expansions of its primary care clinics and the launch of its new insurance arm.
Here are nine numbers that show how big Walmart is in healthcare and how it plans to grow:
Walmart has opened20standalone healthcare centers and plans to open at least 15 more in 2021. The health centers offer primary care, urgent care, labs, counseling and other services.
Walmart’s board approved a plan in 2018 to scale to 4,000clinics by 2029. However, that plan is in flux as the retail giant may be rolling back its clinic strategy, according to a February Insider report.
Walmart in January confirmed plans to offer COVID-19 vaccines in 11 states and Puerto Rico.
In 2020, Walmart established600COVID-19 testing sites.
Walmart said it believes expanding its standalone clinics will help bring affordable, quality healthcare to more Americans because 90 percent of Americans live within 10 miles of a Walmart store.
The Walmart Health model lowers the cost of delivering healthcare services by about 40 percent for patients, according to Walmart’s former health and wellness president Sean Slovenski.
In October, Walmart partnered with Medicare Advantage insurer Clover Health on its first health insurance plans, which will be available to 500,000 people in eight Georgia counties.
Walmart’s insurance arm, Walmart Insurance Services, partnered with eight payers during the Medicare open enrollment period in 2020 to sell its Medicare products. Humana, UnitedHealthcre and Anthem Blue Cross Blue Shield were among the insurers offering the products.
Many physician practices weathered 2020 better than they would have predicted last spring. We had anticipated many doctors would look to health systems or payers for support, but the Paycheck Protection Program (PPP) loans kept practices going until patient volume returned. But as they now see an end to the pandemic, many doctors are experiencing a new round of uncertainty about the future. Post-pandemic fatigue, coupled with a long-anticipated wave of retiring Baby Boomer partners, is leading many more independent practices to consider their options. And layered on top of this, private equity investors are injecting a ton of money into the physician market, extending offers that leave some doctors feeling, according to one doctor we spoke with, that“you’d have to be an idiot to say no to a deal this good”.
2021 is already shaping up to be a record year for physician practice deals.Butsome of our recent conversations made us wonder if we had time-traveled back to the early 2000s, when hospital-physician partnerships were dominated by bespoke financial arrangements aimed at securing call coverage and referrals. Some health system leaders are flustered by specialist practices wanting a quick response to an investor proposal. Hospitals worry the joint ventures or co-management agreements that seemed to work well for years may not be enough, and wonder if they should begin recruiting new doctors or courting competitors, “just in case” current partners might jump ship for a better deal.
In contrast to other areas of strategy, where a ten-year vision can guide today’s decisions, it has always been hard for health systems to take the long view with physician partnerships.
When most “strategies” are really just responses to the fires of the day, health systems run the risk of relationships devolving to mere economic terms.Health systems may find themselves once again with a messy patchwork of doctors aligned by contractual relationships, rather than a tight network of physician partners who can work together to move care forward.
COVID-19 accelerated a number of trends already brewing in the healthcare industry, and that’s not likely to change this year, according to a new report from CVS Health.
The healthcare giant released its annual Health Trends Report on Tuesday, and the analysis projects several industry trends that are likely to define 2021 in healthcare, ranging from technology to behavioral health to affordability.
“We are facing a challenging time, but also one of great hope and promise,” CVS CEO Karen Lynch said in the report. “As the pandemic eventually passes, its lessons will serve to make our health system more agile and more responsive to the needs of consumers.”
Here’s a look at four of CVS’ predictions:
1. A looming mental health crisis
Behavioral health needs were a significant challenge in healthcare prior to COVID-19, but the number of people reporting declining mental health jumped under the pandemic.
Cara McNulty, president of Aetna Behavioral Health, said in a video attached to the report that it will be critical to “continue the conversation around mental health and well-being” as we emerge from the pandemic and to reduce stigma so people who need help seek it out.
“We’re normalizing that it’s important to take care of our mental well-being,” she said.
Data released in December by GoodRx found that prescription fills for depression and anxiety medications hit an all-time high in 2020. GoodRx researchers polled 1,000 people with behavioral health conditions on how they were navigating the pandemic, and 63% said their depression and/or anxiety symptoms worsened.
McNulty said symptoms to look for when assessing whether someone is struggling with declining mental health include whether they’re withdrawn or agitated or if there’s a notable difference in their self-care routine.
2. Pharmacists take center stage
CVS dubbed 2021 “the year of the pharmacist” in its report.
The company expects pharmacists to be a key player in a number of areas, especially in vaccine distribution as that process inches toward broader access. They also offer a key touchpoint to counsel patients about their care and direct them to appropriate services, CVS said.
CVS executives said in the report that they see a significant opportunity for pharmacists to have a positive impact on the social determinants of health.
“We’ve found people are not only open and willing to share social needs with their pharmacists but in many cases, they listen to and act on the advice and recommendations of pharmacists,” Peter Simmons, vice president of transformation, pharmacy delivery and innovation at CVS Health, said in the report.
3. Finding ways to mitigate the cost of high-price therapies
Revolutionary drugs and therapies are coming to market with eye-popping price tags; it’s not uncommon to see new pharmaceuticals priced at $1 million or more. For pharmacy benefit managers, this poses a major cost challenge.
To address those prices, CVS expects value-based contracting to take off in a big way. And drugmakers are comfortable with the idea, according to the report. Novartis, for example, is offering insurers a five-year payment plan for its $2 million gene therapy Zolgensma, with refunds available if the drug doesn’t achieve desired results.
CVS said the potential for these therapies is clear, but many payers want to see some type of results before they fork over hundreds of thousands.
“Though the drug may promise to cure these patients for life, these are early days in their use,” said Joanne Armstrong, M.D., enterprise head of women’s health and genomics at CVS Health, in the report. “What we’re saying is, show us the clinical value proposition first.”
CVS said it’s also offering a stop-loss program for gene therapy to self-funded employers contracted with Aetna and/or Caremark to assist them in capping the expenses associated with these drugs.
4. Getting into the community to address diabetes
Diabetes risk is higher among vulnerable populations, such as Black patients, and addressing it will require local and community-based solutions, CVS executives said in the report. Groups at the highest risk for the disease are less likely to live in areas with easy access to a supermarket, for example, which boosts their risk of unhealthy eating, according to the report.
The two key hurdles to addressing this issue are access and affordability. The rise in retail clinics and ambulatory care centers can get at the access issue, as they can offer a way to better meet patients where they are.
At CVS’ MinuteClinics, patients can walk in and receive a number of services to assist them in managing diabetes, including screenings, consultations with providers and connections to diabetes educators who can assist with lifestyle changes.
Retail locations can also assist with medication costs, creating a one-stop-shop experience that’s easier for many diabetes patients to slot into their daily lives, CVS said.
“Diabetes is a case study in how a more connected experience can translate to simpler, affordable and more accessible care for underserved communities,” said Dan Finke, executive vice president of CVS Health and president of its healthcare benefits division.
UnitedHealth subsidiary Optum signed a definitive agreement to acquire Atrius Health, a 715-physician group based in Newton, Mass., according to The Boston Globe.
Optum said March 2 the agreement was signed the evening of March 1 after UnitedHealth’s board approved the transaction. Atrius’ board also unanimously approved the deal.
The deal will need approval from Massachusetts’ Health Policy Commission, the Department of Public Health and the Federal Trade Commission.
If the deal is approved, it would expand Optum’s presence in Massachusetts. The organization had previously acquired Worcester, Mass.-based Reliant Medical Group in April 2018.
Optum reportedly had been interested in purchasing Atrius, which has 30 locations in Massachusetts, for a few years and submitted a bid for it in 2019 when the medical group was looking for a partner. In 2019, Atrius decided to remain independent. However, Atrius said it decided to reignite potential partnership talks again due to the pressures of the pandemic.
“We looked at many alternatives and chose [Optum] because of cultural alignment, the benefit we could provide for patients, the stability it could provide for our practice, and the help we can provide to the commonwealth as it pertains to managing medical spend,” Atrius President and CEO Steven Strongwater, MD, told the Boston Business Journal.
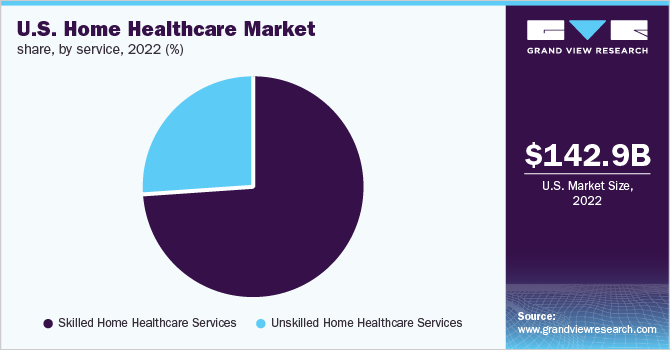
This week Brookdale Senior Living, the nation’s largest operator of senior housing, with 726 communities across 43 states and annual revenues of about $3B, announced the sale of 80 percent of its hospice and home-based care division to hospital operator HCA Healthcare for $400M. The transaction gives HCA control of Brookdale’s 57 home health agencies, 22 hospice agencies, and 84 outpatient therapy locations across a 26-state footprint, marking its entry into new lines of business, and allowing it to expand revenue streams by continuing to treat patients post-discharge, in home-based settings.
Like other senior living providers, Brookdale has struggled economically during the COVID pandemic; its home and hospice care division, which serves 17,000 patients, saw revenue drop more than 16 percent last year. HCA, meanwhile, has recovered quickly from the COVID downturn, and has signaled its intention to focus on continued growth by acquisition across 2021.
In separate news, Optum, the services division of insurance giant UnitedHealth Group, was reported to have struck a deal to acquire Landmark Health, a fast-growing home care company whose services are aimed at Medicare Advantage-enrolled, frail elderly patients. Landmark, founded in 2014, also participates in Medicare’s Direct Contracting program.
The transaction is reportedly valued at $3.5B, although neither party would confirm or comment on the deal. The acquisition would greatlyexpand Optum’s home-based care delivery services, which today include physician home visits through its HouseCalls program, and remote monitoring through its Vivify Health unit.
The Brookdale and Landmark deals, along with earlier acquisitions by Humana and others, indicate that the home-based care space is heating up significantly,reflecting a broader shift in the nexus of care to patients’ homes—a growing preference among consumers spooked by the COVID pandemic.
Along with telemedicine, home-based care may represent a new front in the tug-of-war between providers and payers for the loyalty of increasingly empowered healthcare consumers.
Even though signs point to a post-COVID spike in health system mergers, retailers, insurers, and other healthcare industry players already far exceed health system scale. Even the largest of the “mega health systems” pale in comparison to other healthcare companies up and down the value chain, as shown in the graphic above. And with the exception of pharma, these other industry players have seen revenues surge during the pandemic, while health system growth has stagnated.
According to a recent report from Kaufman Hall, hospitals saw a three percent reduction in annual total gross revenue in 2020.The majority of the decrease stemmed from a six percent decline in outpatient revenue, as volumes plummeted during the pandemic.
The largest companies listed here, including Walmart, Amazon, CVS, and UnitedHealth Group, continue to double down on vertical integration strategies, configuring an array of healthcare assets into platform businesses focused on delivering value to consumers.
To remain relevant, health systems will need to increase their focus on this strategy as well, assembling the right capabilities for a marketplace driven by value, at a scale that enables rapid innovation and sustainability.
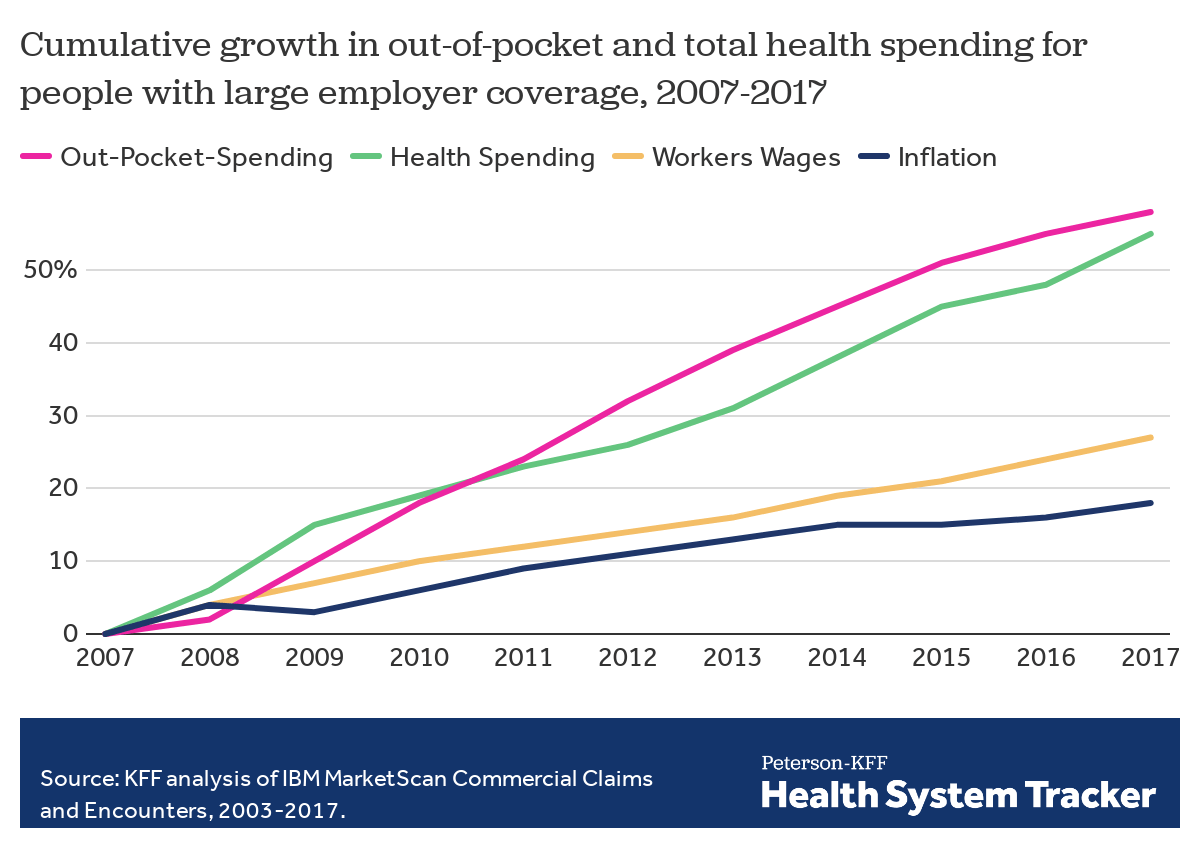
Employers — including companies, state governments and universities — purchase health care on behalf of roughly 150 million Americans. The cost of that care has continued to climb for both businesses and their workers.
For many years, employers saw wasteful care as the primary driver of their rising costs. They made benefits changes like adding wellness programs and raising deductibles to reduce unnecessary care, but costs continued to rise. Now, driven by a combination of new research and changing market forces — especially hospital consolidation — more employers see prices as their primary problem.
By amassing and analyzing employers’ claims data in innovative ways, academics and researchers at organizations like the Health Care Cost Institute (HCCI) and RAND have helped illuminate for employers two key truths about the hospital-based health care they purchase:
1) PRICES VARY WIDELY FOR THE SAME SERVICES
Data show that providers charge private payers very different prices for the exact same services — even within the same geographic area.
For example, HCCI found the price of a C-section delivery in the San Francisco Bay Area varies between hospitals by as much as:$24,107
Data show that hospitals charge employers and private insurers, on average, roughly twice what they charge Medicare for the exact same services. A recent RAND study analyzed more than 3,000 hospitals’ prices and found the most expensive facility in the country charged employers:4.1xMedicare
Hospitals claim this price difference is necessary because public payers like Medicare do not pay enough. However, there is a wide gap between the amount hospitals lose on Medicare (around -9% for inpatient care) and the amount more they charge employers compared to Medicare (200% or more).
Employer Efforts
A small but growing group of companies, public employers (like state governments and universities) and unions is using new data and tactics to tackle these high prices. (Learn more about who’s leading this work, how and why by listening to our full podcast episode in the player above.)
Note that the employers leading this charge tend to be large and self-funded, meaning they shoulder the risk for the insurance they provide employees, giving them extra flexibility and motivation to purchase health care differently. The approaches they are taking include:
Steering Employees
Some employers are implementing so-called tiered networks, where employees pay more if they want to continue seeing certain, more expensive providers. Others are trying to strongly steer employees to particular hospitals, sometimes know as centers of excellence, where employers have made special deals for particular services.
Purdue University, for example, covers travel and lodging and offers a $500 stipend to employees that get hip or knee replacements done at one Indiana hospital.
Negotiating New Deals
There is a movement among some employers to renegotiate hospital deals using Medicare rates as the baseline — since they are transparent and account for hospitals’ unique attributes like location and patient mix — as opposed to negotiating down from charges set by hospitals, which are seen by many as opaque and arbitrary. Other employers are pressuring their insurance carriers to renegotiate the contracts they have with hospitals.
In 2016, the Montana state employee health plan, led by Marilyn Bartlett, got all of the state’s hospitals to agree to a payment rate based on a multiple of Medicare. They saved more than $30 million in just three years. Bartlett is now advising other states trying to follow her playbook.
In 2020, several large Indiana employers urged insurance carrier Anthem to renegotiate their contract with Parkview Health, a hospital system RAND researchers identified as one of the most expensive in the country. After months of tense back-and-forth, the pair reached a five-year deal expected to save Anthem customers $700 million.
Legislating, Regulating, Litigating
Some employer coalitions are advocating for more intervention by policymakers to cap health care prices or at least make them more transparent. States like Colorado and Indiana have passed price transparency legislation, and new federal rules now require more hospital price transparency on a national level. Advocates expect strong industry opposition to stiffer measures, like price caps, which recently failed in the Montana legislature.
Other advocates are calling for more scrutiny by state and federal officials of hospital mergers and other anticompetitive practices. Some employers and unions have even resorted to suing hospitals like Sutter Health in California.
Employer Challenges
Employers face a few key barriers to purchasing health care in different and more efficient ways:
Provider Power
Hospitals tend to have much more market power than individual employers, and that power has grown in recent years, enabling them to raise prices. Even very large employers have geographically dispersed workforces, making it hard to exert much leverage over any given hospital. Some employers have tried forming purchasing coalitions to pool their buying power, but they face tricky organizational dynamics and laws that prohibit collusion.
Sophistication
Employers can attempt to lower prices by renegotiating contracts with hospitals or tailoring provider networks, but the work is complicated and rife with tradeoffs. Few employers are sophisticated enough, for example, to assess a provider’s quality or to structure hospital payments in new ways.Employers looking for insurers to help them have limited options, as that industry has also become highly consolidated.
Employee Blowback
Employers say they primarily provide benefits to recruit and retain happy and healthy employees. Many are reluctant to risk upsetting employees by cutting out expensive providers or redesigning benefits in other ways. A recent KFF survey found just 4% of employers had dropped a hospital in order to cut costs.
The Tradeoffs
Employers play a unique role in the United States health care system, and in the lives of the 150 million Americans who get insurance through work. For years, critics have questioned the wisdom of an employer-based health care system, and massive job losses created by the pandemic have reinforced those doubts for many.
Assuming employers do continue to purchase insurance on behalf of millions of Americans, though, focusing on lowering the prices they pay is one promising path to lowering total costs. However, as noted above, hospitals have expressed concern over the financial pressures they may face under these new deals. Complex benefit design strategies, like narrow or tiered networks, also run the risk of harming employees, who may make suboptimal choices or experience cost surprises. Finally, these strategies do not necessarily address other drivers of high costs including drug prices and wasteful care.
With nearly 30% of workers now having a high deductible health plan and a typical family being responsible for on average the first $8,000 of costs, consumers are increasingly weighing care versus cost. Historically, with a small copay, you would conveniently take care of an ailment without shopping around, but with the average person now bearing the brunt of the initial costs, wouldn’t you want to know how much a service costs and what other providers are charging before you “buy” the service?
CMS believes“consumers should be able to know, long before they open a medical bill, roughly how much a hospital will charge for items and services it provides.” Cue the hospital price transparency rule that just went into effect January 1, 2021. Hospitals are now required to post their standard charges, including the rates they negotiate with insurers, and the discounted price a hospital is willing to accept directly from a patient if paid in cash. As a consumer, the intent is to make it “easier to shop and compare prices across hospitals and estimate the cost of care before going to the hospital.”
There are a few different angles to analyze here:
Are hospitals following the rules?
Each hospital must post online a comprehensive machine readable file with all items and services, including gross charges, actual negotiated prices with insurers, and the cash price for patients who are uninsured. Additionally, hospitals must post the costs for 300 common “shoppable” services in a “consumer-friendly format.” Some hospitals and health systems have done a good job at posting these prices in a digestible format, like the Cleveland Clinic or Sutter Health, but others have posted complicated spreadsheets, relied on online cost estimator tools, or simply not posted them at all. An analysis from consulting firm ADVI of the top 20 largest hospitals in the U.S. found that not all of them appeared to completely comply with this mandate. In some instances, data was not able to be downloaded in a useable format, others did not post the DRG or service codes, and the variability in the terms/categories used simply created difficulty in comparing pricing information across hospitals. CMS has stated that a failure to comply with the rules could result in a fine of up to $300 per day. As with most new rules, there are growing pains, and hospitals will likely get better at this over time, assuming the data is being used for its original intent.
Is this helpful to consumers?
Consumers will able to see the variation in prices for the exact same service or procedure between hospitals and get an estimate of what they will be charged before getting the care. But how likely is the average person to go to their hospital’s website, look at a price, and change their decision about where to get care? In addition, awareness of these price transparency tools is still low among consumers. Frankly, it is competitors and insurers that have been first in line to review the data. Looking through a number of hospital websites, and even certain state agency sites that have done a good job at summarizing the costs, like Florida Health Price Finder, the price transparency tools are helpful, but appear to be much more suited for relatively standardized services that can be scheduled in advance, like a knee replacement. It’s highly unlikely you will be telling your ambulance driver what hospital to go to based on cost while in cardiac arrest…Plus, it’s all still confusing – even physicians have shared their bewilderment, when trying to decipher and compare pricing. Conceptually, price transparency should be beneficial to consumers, but it will take time; and it will need to involve not just the hospitals posting rates, but the outpatient care facilities as well. Knowing what you will pay before you decide to go to a physician’s office or a clinic or an urgent care or an ED will hopefully help drive consumers to make more educated decisions in the future.
Will this ultimately drive down costs?
I sure hope so. Revealing actual negotiated prices between hospitals and insurers should push the more expensive hospitals in the area to reduce prices, especially if consumers start using the other hospitals, instead. However, it could also have an inverse effect, with lower cost hospitals insisting on a payment increase from insurers; thereby driving up costs. In the end, as has historically been the case, the market power of certain providers will likely dictate the direction of costs in a given region. That is, until both price AND quality become fully transparent and the consumer is armed with the tools to shop for the best care at the lowest cost – consumerism here we come.
Molina’s net income fell sharply in the fourth quarter as the insurer was forced to refund rates to some of its state partners as COVID-19 continues to depress normal care utilization, CEO Joe Zubretsky told investors Thursday.
Although utilization remained curtailed, COVID-19 costs were higher in the fourth quarter than any other quarter in 2020, Zubretsky said. As such, Molina’s medical care ratio for the quarter increased to 90.8% from 86% the prior-year period.
Still, Molina remained in the black for the full year of 2020. Looking ahead, the company expects utilization to improve, though does not expect it to rebound entirely. At the same time, the company expects direct COVID-19 costs to come in lower than last year.
Dive Insight:
Insurers have largely remained unbruised from the pandemic, unlike some providers, but the fourth quarter was a different story.
The pandemic took a bite out of Molina’s net income in the fourth quarter as the company reported that figure fell to $34 million from $168 million in Q4 2019.
The biggest contributor to the impact on the bottom line was Medicaid refunds to states, including California, Michigan and Ohio. States have clawed back some of the money they pay insurers like Molina as members continue to defer care, which is a benefit to insurers as they then pay out less.
Molina painted a clearer picture of this scenario during Thursday’s conference call with investors.
For the full year, Molina estimated that medical cost suppression amounted to $620 million while direct COVID-19 costs amounted to $200 million. In other words, curbed utilization continued to outweigh direct COVID-19 costs, resulting in a $420 million benefit from the pandemic, which the company characterized as a surplus.
But states took back a total of $565 million through rate refunds. Overall, the net impact of COVID-19 was a $180 million hit to Molina for 2020 when factoring in other costs.
Looking ahead, executives seemed cautiously optimistic for 2021 but noted headwinds from the pandemic will persist. While the forecast reflects future growth, Zubretsky said, “it is a constrained picture” of the company’s potential earnings.
Some of those headwinds include Medicare risk scores that don’t fully capture the acuity of their Medicare members. As seniors put off care in 2020, companies like Molina were unable to capture diagnosis codes to help them determine how sick members are and the ultimate risk they pose.
Still, there are some bright spots. As the public health emergency is likely to be continued throughout the remainder of the year, it means that redeterminations will remain halted, or, in other words, Medicaid members will not be kicked off coverage.
This was a boon for Molina in 2020, as it allowed them to pick up a significant number of new members. Overall, it was a major catalyst for Medicaid membership growth in 2020, Zubretsky said.
Molina expects care utilization to improve this year but not fully return to normal. Instead, it expects utilization suppression to be about one third of 2020 levels.
Molina, which solely focuses its portfolio on government sponsored and marketplace plans, said it expects to pick up as many as 30,000 additional members during the Affordable Care Act special enrollment period.
Opening up a special enrollment period was one of the first moves made by the new administration in the White House. Zubretsky seems enthused by the recent moves through executive orders and the unfolding bill developments in Congress that are looking to raise premium subsidies on the exchanges.
Those early actions “just couldn’t be better for government sponsored managed care, and we’re pleased to see that progress already being made,” Zubretsky said.