The healthcare industry is still licking its wounds from $1 trillion in federal funding cuts included in the One Big Beautiful Bill Act (OBBBA) signed into law July 4.
Adding insult to injury, the Center for Medicare and Medicaid services issued a 913-page proposed rule last Tuesday that includes unwelcome changes especially troublesome for hospitals i.e. adoption of site neutral payments, expansion of hospital price transparency requirements, reduction of inpatient-only services, acceleration of hospital 340B discount repayment obligations and more.
The combination of the two is bad news for healthcare overall and hospitals especially: the timing is precarious:
Economic uncertainty: Economists believe a recession is less likely but uncertainty about tariffs, fear about rising inflation, labor market volatility a housing market slowdown and speculation about interest rates have capital markets anxious. Healthcare is capital intense: the impact of the two in tandem with economic uncertainty is unsettling.
Consumer spending fragility: Consumer spending is holding steady for the time being but housing equity values are dropping, rents are increasing, student loan obligations suspended during Covid are now re-activated, prices for hospital and physicians are increasing faster than other necessities and inflation ticked up slightly last month. Consumer out-of-pocket spending for healthcare products and services is directly impacted by purchases in every category.
Heightened payer pressures: Insurers and employers are expecting double-digit increases for premiums and health benefits next year blaming their higher costs on hospitals and drugs, OBBBA-induced insurance coverage lapses and systemic lack of cost-accountability. For insurers, already reeling from 2023-2024 financial reversals, forecasts are dire. Payers will heighten pressure on healthcare providers—especially hospitals and specialists—as a result.
Why healthcare appears to have borne the brunt of the funding cuts in the OBBBA is speculative:
Might a case have been made for cuts in other departments? Might healthcare programs other than Medicaid have been ripe for “waste, fraud and abuse” driven cuts? Might technology-driven administrative costs reductions across the expanse of federal and state government been more effective than DOGE- blunt experimentation?
Healthcare is 18% of the GDP and 28% of total federal spending: that leaves room for cuts in other industries.
Why hospitals, along with nursing homes and public health programs, are likely to bear the lion’s share of OBBBA’ cut fallout and CMS’ proposed rule disruptions is equally vexing. Might the high-profile successes of some not-for-profit hospital operators have drawn attention? Might Congress have been attentive to IRS Form 990 filings for NFP operators and quarterly earnings of investor-owned systems and assume hospital finances are OK? Might advocacy efforts to maintain the status quo with facility fees, 340B drug discounts, executive compensation et al been overshadowed by concerns about consolidation-induced cost increases and disregard for affordability? Hospital emergency rooms in rural and urban communities, nursing homes, public health programs and many physicians will be adversely impacted by the OBBBA cuts: the impact will vary by state. What’s not clear is how much.
My take:
Having read both the OBBBA and CMS proposed rules and observed reactions from industry, two things are clear to me:
The antipathy toward the healthcare industry among the public and in Congress played a key role in passage of the OBBBA and regulatory changes likely to follow.
Polls show three-fourths of likely voters want to see transformational change to healthcare and two-thirds think the industry is more concerned with its profit over their care: these views lend to hostile regulatory changes. The public and the majority of elected officials think the industry prioritizes protection of the status quo over obligations to serve communities and the greater good.
The result: winners and losers in each sector, lack of continuity and interoperability, runaway costs and poor outcomes.
No sector in healthcare stands as the surrogate for the health and wellbeing of the population. There are well-intended players in each sector who seek the moral high ground for healthcare, but their boards and leaders put short-term sustainability above long-term systemness and purpose. That void needs to be filled.
The timing of these changes is predictably political.
Most of the lower-cost initiatives in both the OBBBA changes and CMS proposals carry obligations to commence in 2026—in time for the November 2026 mid-term campaigns. Most of the results, including costs and savings, will not be known before 2028 or after. They’re geared toward voters inclined to think healthcare is systemically fraudulent, wasteful and self-serving.
And they’re just the start: officials across the Departments of Health and Human Services, Justice, Commerce, Labor and Veterans Affairs will add to the lists.
Last Thursday, the Make America Healthy Again Commission released its 68-page report “Making America’s Children Healthy Again Assessment” featuring familiar themes—the inadequacy of attention to chronic disease by the health system, the “over-medicalization” of patient care vis a vis prescription medicines et al, the contamination of the food-supply by harmful ingredients, and more.
HHS Secretary Kennedy, EPA Administrator Zeldin and Agriculture Secretary Rollins pledged war on the corporate healthcare system ‘that has failed the public’ and an all-of-government approach to remedies for burgeoning chronic care needs.
Also Thursday, the House of Representatives passed its budget reconciliation bill by a vote of 215-214. The 1000-page bill cuts federal spending by $1.6 trillion (including $698 billion from Medicaid) and adds $2.3 trillion (CBO estimate/$3.4 to $5 trillion per Yale Budget Lab) to the national deficit over the next decade. It now goes to the Senate where changes to reduce federal spending to pre-pandemic level will be the focus.
With a 53-37 advantage and 22 of the 36 Senate seats facing mid-term election races in November, 2026, the Senate Republican version of the “Big Beautiful Bill” will include more spending cuts while pushing more responsibility to states for funding and additional cuts. The gap between the House and Senate versions will be wider than currently anticipated by House Republicans potentially derailing the White House promise of a final Big Beautiful Bill by July 4.
And, over the last week and holiday weekend, the President announced a new 25% tariff on Apple devices manufactured in India and new tariffs targeting the EU; threatened cuts to federal grants to Harvard and cessation of its non-citizen student enrollment, a ‘get-tougher’ policy on Russia to pressure an end of its Ukraine conflict, and a pledge to Americans on Memorial that it will double down on ‘peace thru strength’ in its Make America Great Again campaign.
These have 2 things in common:
1-They’re incomplete. None is a finished product.
The MAHA Commission, working with the Departments of Health & Human Services, Interior and Agriculture, is tasked to produce another report within 90 days to provide more details about a plan. The FY26 budgeting process is wrought with potholes—how to satisfy GOP deficit hawks vs. centrist lawmakers facing mid-term election, how to structure a bill that triggers sequestration cuts to Medicare (projected $490 billion/10 yrs. per CBO), how to quickly implement Medicaid work requirements and marketplace enrollment cuts that could leave insurance coverage for up to 14 million in limbo, and much more. And the President’s propensity to “flood the zone” with headline-grabbing Truth Social tweets, Executive Orders and provocative rhetoric on matters at home and abroad will keep media occupied and healthcare spending in the spotlight.
2-They play to the MAGA core.
The MAGA core is primarily composed of older, white, Christian men driven by a belief that the United States has lost its exceptionalism through WOKE policies i.e. DEI in workplaces and government, open borders, globalization and excessive government spending and control. In the 2024 Presidential election, the MAGA core expanded incrementally among Black, Hispanic, and younger voters whose concerns about food, energy and housing prices prompted higher-than expected turnout. The MAGA core believes in meritocracy, nationalism, smaller government, lower taxes, local control and free-market policies that encourage private investment in the economy. The core is price sensitive.
The health system per se is not a concern but it’s the affordability and lack of price transparency are. They respect doctors and frontline caregivers but think executives are overpaid and prone to self-promotion. And the MAGA core think lawmakers have been complicit in the system’s lack of financial accountability largely beneficial to elites.
Looking ahead to the summer, a “Big Beautiful Bill” will pass with optics that allow supporters to claim fiscal constraint and lower national debt and opponents to decry insensitive spending cuts and class warfare against low-and-middle-class households.
Federal cuts to Medicaid and SNAP (Supplemental Nutrition Assistance Program) will be prominent targets in both groups—one a portrayal of waste, fraud and abuse and the other tangible evidence of societal inequity and lack of moral purpose. Each thinks the other void of a balanced perspective. Each thinks the health system is underperforming and in need of transformational change but agreement about how to get there unclear.
As MAHA promotes its agenda, Congress passes a budget and MAGA advances its anti-establishment agenda vis a vis DOGE et al, healthcare operators will be in limbo. The dust will settle somewhat this summer, but longer-term bets will be modified for most organizations as compliance risks change, state responsibilities expand, capital markets react and Campaign 2026 unfolds.
And in most households, concern about the affordability of medical care will elevate as federal and state funding cuts force higher out of pocket costs on consumers and demand for lower prices.
The summer will be busy for everyone in healthcare.
PS: Changes in the housing market are significant for healthcare: 36% of the CPI is based on shelter vs. 8% for medical services & products, 14% for food and 6% for energy/transportation. While the overall CPI increased 2.3% in the last 12 months, medical services prices increased 3.1%. contributing to heightened price sensitivity and delayed payments.
It has not escaped lawmaker attention: revenue cycle management business practices (debt collection) are being scrutinized in hospitals and community benefit declarations by not-for-profit hospitals re-evaluated. The economics of healthcare are not immune to broader market trends nor is spending for healthcare in households protected from day-to-day fluctuations in prices for other goods and services.
The U.S. bombing of Iran’s nuclear capability is unsettling: whether MAGA or not, hawk or dove, young or old, conservative or liberal, rich or poor—it matters.
Stability at home and abroad is utopian to some but desired by all. Pandemics, mass violence, natural disasters and even election results contribute to instability and lend to insecurity. Operation Midnight Hammer might contribute to the nation’s anxiety—time will tell.
The immediate aftermath of the bunker-bombings in Iran will involve two orchestrated campaigns by government officials:
The Campaign to Contain Middle East Tension: military, diplomatic and economic levers will be put to the test to limit escalation of the bombing and limit its consequence to the region.
The Campaign to Win Public Support: issues of consequence like military intervention ultimately depend on public opinion that support laws, funding and subsequent actions taken in response. History teaches and political leaders understand that ‘winning the hearts and minds’ of the public is necessary to success. Predictably, justification for Operation Midnight Hammer will be messaged loudly by supporters and challenged by critics.
For the moment, the news cycle will shift to foreign policy and away from tariffs, inflation, household prices and the “Big Beautiful Budget Bill” which the Senate Republicans hope to bring to the floor this week. News media will speculate about the after-effects of the Israeli-Iran bombing and what role the U.S. plays in an increasingly complicated geopolitical landscape marked by marked by armed conflicts Gaza, Ukraine, Myanmar, Yemen and 26 and other countries.
The attention these get in traditional media and social media channels will exacerbate public anxiety that’s already high: 19% U.S. adults and 40% of the country’s adolescents suffer from anxiety disorder: “a persistent, excessive fear or worry that interferes with daily life and functioning”. But, per the National Institute of Mental Health, fewer than a third suffering from severe anxiety receive professional treatment.
In the public health community, much is known about anxiety: it’s more prevalent among women than men, in minority populations, lower income populations and in the Southeast. It’s significant across all age groups, and at an alarming level among young working-class adults facing unique issues like affordability and job insecurity. And it is stigmatized in certain communities (i.e. certain fundamentalist religious sects, certain ethnic communities) lending to silent suffering and unattended consequences.
My take:
Operation Midnight Hammer came at a time of widespread public anxiety about the economy, tariffs, inflation, costs of living and political division. I will let pundits debate the advisability and timing of the bunker-bombing but I know one thing for sure: mental health issues—including anxiety, mood and substance abuse disorders– deserve more support from policymakers and more attention by the healthcare community.
The former requires local, state and federal lawmakers to revisit and enforce mental health parity laws already on the books but rarely enforced.
The latter requires the healthcare community to elevate behavioral health to a national priority alongside obesity, heart disease, cancer and aging to secure the public’s health and avoid unintended consequences of neglect.
Regrettably, the issue is not new. Employers, school systems, religious organizations and local public health agencies have been mental health default safety values to date; extreme have been temporarily shuffled to in hospital emergency rooms most ill-equipped to manage them. But systematic, community-wide, evidence-based help for those in need of mental health remains beyond their reach.
The Trump administration’s healthcare leaders under HHS’ Kennedy and CMS’ Oz espouse the U.S. healthcare system should prioritize chronic disease and preventive health. They believe its proficiency in specialty care is, in part, the result of lucrative incentives that reward providers and their financial backers handsomely in these areas.
In the President’s February 13 Executive Order establishing the Make America Healthy Again Commission, its goal was laid out:
“To fully address the growing health crisis in America, we must re-direct our national focus, in the public and private sectors, toward understanding and drastically lowering chronic disease rates and ending childhood chronic disease. This includes fresh thinking on nutrition, physical activity, healthy lifestyles, over-reliance on medication and treatments, the effects of new technological habits, environmental impacts, and food and drug quality and safety… We must ensure our healthcare system promotes health rather than just managing disease.”
Nothing could be more timely and necessary to the Commission’s work than addressing mass anxiety and mental health as a national priority. And nothing is more urgently needed in communities than mainstreaming anxiety and mental health into the systems of health that accept full risk for whole person health.
PS: Before Operation Midnight Hammer over the weekend, I had prepared today’s report focused on two government reports about the long-term solvency of the Medicaid and Medicare programs. Given the gravity of events in Israel and Iran and other hot spots, and after discussions with my family and friends this weekend, it became clear public anxiety is high.
I am concerned about the future and worry about the health system’s response. It’s composed of good people doing worthwhile work who are worried about the future. I recently spoke to a group on the theme (link below): ‘the future for healthcare is not a repeat of its past.’ That lends to anxiety unless accompanied by a vision for a better future. That’s what all hope for those in Iran, Gaza, Israel and beyond, and for all who serve in our industry.
Hi, everybody. I’m Elizabeth Wilkins, president and CEO of the Roosevelt Institute, and I am delighted to be here today with some big news and a very special guest. I am thrilled to announce that Nobel Prize–winning economist Paul Krugman will be joining the Roosevelt Institute as a senior fellow. Paul is one of the world’s most cited economists and widely read commentators, and for good reason. His longtime New YorkTimes column and his Substack now prove that he is not just a bold thinker, he is one of the clearest and most dynamic communicators in the field—skills that come in handy when you want to break through the noise of this moment and get people thinking about what the future of our economy and democracy might look like. And, of course, this is what Roosevelt is all about: understanding where we are in the moment and where we need to go.
So, Paul, I’m so excited to talk with you today. I started at Roosevelt in February, so we’re both new kids on the block here, and I will start with a question that I am getting a lot recently: Why your interest in affiliating with Roosevelt, and why now?
Paul Krugman:
Well, now I think because partly having retired from the New York Times, I’m free to pursue other affiliations. The Times is kind of a jealous organization. But now that I’m no longer there, I can do this. Roosevelt has been a tremendous reservoir of progressive thinking and progressive economics. I was heavily reliant on Roosevelt research particularly during the aftermath of the 2008 financial crisis—I’ve been around for a while here. [There’s] still novel stuff going on, and this seemed like a good affiliation to have in these times, to join the ranks of people with Roosevelt affiliations who have been providing really urgent commentary.
Elizabeth:
Thank you for the kind words. We appreciate it. One of the things that made your Times column such a hit for decades was the unique voice that you bring to economics: your ability to break down orthodoxy and cut to the core of what’s happening in plain terms. It almost goes without saying that there is a lot to cut through right now. We’ve seen attacks on government programs and on whole government agencies. And as you have noted and I have noted, the fate of Social Security and our social compact hangs in the balance right now. So, can you talk—with a little bit of your perspective on economic history—about what you think makes this moment unique? And through all this noise, what people should be paying attention to, and why?
Paul:
We are in a moment where we’ve lived, really since the New Deal in—whatever you want to call it—the Keynesian consensus. We’ve lived in a world where, we by no means went to socialism, but we had capitalism with some of the rough edges sanded off. Not as many of the rough edges that I would like, but we have Social Security, we’ve had Medicare since the 60s. We have Medicaid. We have the Affordable Care Act. We have a whole bunch of social insurance programs. We have government efforts to at least somewhat regulate the excesses and harms of markets. And now we are at a moment where there’s a real possibility that we may really lose that. We’re talking about possible retrogression, and the possibility of moving forward after this current moment has passed. But we really are at a point where the certainties of the underlying continuity of a fairly decent social compact is at risk. And so this is really new.
Elizabeth:
I really like that phrase, this “capitalism with the rough edges sanded off.” And what I’m hearing you say is basically the idea of the social compact is that, yes, we have capitalism, but we also have a commitment to providing a measure of security for people, and that’s the deal we have struck. You write a ton about the New Deal and FDR [Franklin D. Roosevelt]. Can you just expand a little bit about how to think about that trade-off, how long that consensus has held, and if there are any other moments in our economic history where there have been similar threats to that compact that we can learn from?
Paul:
I like to think about—it’s 1933, and the world economy has collapsed. There are a lot of reasonable people [who] have concluded that capitalism is irredeemable and can’t be saved, and that on the other hand, you have a lot of forces of repression out there. And along comes several countries—with the US in some ways leading the New Deal order, which says, no, we’re not actually going to go socialist. We’re not going to seize the commanding heights of production, but we are going to try to make sure that extreme hardship is vanished, as far as we can manage. We’re going to try to make sure that workers feel that they are a part of, and that they have rights and claims to, the system. There was very much this moment when we reached a kind of—I don’t know if it’s a compromise or a synthesis—but the idea of a basic standard of decency, the Four Freedoms. While at the same time saying that it’s not evil to make profits. It’s not evil to be personally ambitious. But we are going to try to make it so that everyone shares in the gains from economic activity.
And that really held. I mean, there was the moment when the Reagan administration came in, which represented, in many ways, a turn away from that New Deal consensus. But not to the extent that we have now. In moments of economic stress, people tend to say, well, maybe this thing doesn’t work anymore. The 1970s with stagflation, the aftermath of the 2008 financial crisis. That has basically been the case during attempts to turn away from the basic structure (which in the US context have always been a turn to the right, but in principle, you could imagine a turn to the left, but that hasn’t ever really happened in this country). And until right now, it has always seemed that the public wouldn’t stand for it. When push came to shove, when George W. Bush tried to privatize Social Security, it was a sort of resounding, “no, you don’t. We love Social Security.” But the possibility that we will have either explicitly or de facto undermining of those institutions seems much higher right now just because we live in such—well, we’re not gonna talk about the politics particularly, but there’s a possibility that we’ll lose it, that it will go away. And the one thing that I would say is that there’s this political action by itself, but there’s also the importance of getting the facts clear, getting the way the world works clear. No, there are not 10 million dead people receiving Social Security benefits. No, tax cuts and deregulation are not the only way to achieve economic growth. These are really critical things. Facts matter, analysis matters.
Elizabeth:
I’m just gonna pick up on that last thing you said about facts matter, analysis matters, and maybe go a little bit toward your true economist side. It’s not just Social Security we’re talking about. As you know and just mentioned, we’re in the middle of a tax and budget fight where we are very much looking at a situation where tax cuts for the wealthy might be traded for cuts to the programs that are specifically for our most vulnerable, like Medicaid and SNAP. This obviously has both political economy and democratic implications. It also has economic implications. Can you talk a little bit about this idea of what it means—this kind of wealth transfer, frankly, from the poorest to the richest, both in terms of hard facts, economics, and growth? And in terms of the social compacts that we’ve been talking about.
Paul:
It’s become increasingly clear that taking care of the most vulnerable members of society—it’s something you should do. It’s a moral obligation. But it’s also good economics, especially by the way of children. If you ask, a dollar spent on ensuring adequate health care and nutrition for children clearly pays off with multiple dollars of economic performance, because those children grow up to be more productive adults.
One way to say this is that conservative economic doctrine is all about punishing, it’s all about incentives: Poverty should be painful and wealth should be glorious. And what that all misses is the importance of just plain resources. That if low-income families cannot devote the resources to their children that you need to make those children fully productive adults—some will manage despite that, but just plain making sure that everybody in the country has the resources to make the most of themselves and their children is an enormously practical thing. It’s not just soft-hearted liberal talk, though I am a soft-hearted liberal, but it’s also just what you need to do if you want to make the most of your country’s potential.
Elizabeth:
I’m going to take another policy area, one actually that you know a lot about. It’s the area of focus that won you your Nobel Prize. You, in recent months, have been saying that one of the biggest risks of the Trump administration’s economic agenda is their chaotic tariff policy. We are currently recording the day after Liberation Day. And last year you predicted that the cronyism of those tariffs might be the biggest story in the long run, in addition to the chaos. So can you walk us through those risks, the chaos and the cronyism, and to what degree you’re seeing that play out for American workers and consumers? And, you know, why—I mean, there’s a lot of reasons why—but why are these tariffs different than the years that we’ve seen them in the past?
Paul:
There’s a standard economics case against tariffs, which is that it basically leads your economy to turn away from the things it’s really good at and start doing the things that it’s not especially good at. So for example, in New York, there’s lots of memories of the garment industry, but we really don’t wanna bring the garment industry back. Those were pretty bad jobs, and it happens to be stuff that can be done—where they can do it reasonably well—in Bangladesh, which desperately needs that industry, and we should be doing the things that we’re really good at instead. So that’s the classic case. What we’re discovering is that the rise of this hostility toward trade has additional costs. And the most immediate one is just plain that we don’t know what it’s gonna be.
As you said, we’re recording this the day after Liberation Day, which—nobody knows. I have to say that the actual tariff announcement shocked a lot of people, because it was both much bigger and much more arbitrary than people expected. I wouldn’t have been really shocked if there was a 15 percent across-the-board tariff, because that had been foreshadowed. But instead, there’s different tariffs for every country and this wasn’t really on anybody’s playbook. And nobody knows whether it [will] persist.
Think of yourself as being a business person trying to make decisions. You’re going to make an investment in your business—or are you? I mean, should you be spending money and making commitments on the basis that, okay, we’re gonna have 20 percent tariffs on all goods from Europe, or should you make it on the proposition that, “look, that’s crazy, those won’t last”? And both of those are defensible propositions. Anything you do, if you invest on the assumption that the tariffs are here to stay, then you’ll have made a terrible decision if they don’t. And so there’s a lot of paralysis that comes from the chaos. I’ve always been skeptical of people who invoke uncertainty as a reason that policy is holding the economy back, but because it’s often used as an argument against progressive policies: Oh, you know, your universal health care goals, that creates uncertainty. But in this case, this really is a major harmful issue.
We have not yet seen the cronyism, but it’s clearly potential. The whole root of—the reason why trade is where the dramatic stuff is happening [is because] US law creates a lot of discretion for the executive branch in tariff setting. Tariffs were only supposed to be applied as remedies for specific kinds of shocks or specific kinds of threats, but the decision about whether those conditions apply lies with the executive branch. So a president who wants to can do whatever they want on trade. And in the past, that’s always been held back by concern about: How will other countries react? What about the system? We built this global trading system. So it’s always been assumed that the president would have a wider view.
But if you take that away, then it’s not just arbitrary in terms of what are the overall levels of tariffs, it’s who gets a tariff break. And in fact, every time we do impose tariffs, there tend to be some exemptions. There are good reasons why sometimes you might want to exempt somebody from a tariff. But if it’s all arbitrary, the exemption might come because you go golfing with the president. And so that creates a lot of problematic incentives. We actually saw that in 2017, 2018, when the US was putting on tariffs—which looked trivial compared to what’s now on the plate—but it was very clear that industries and companies that were politically tied to the administration in power were much more likely to get exemptions than those that weren’t. So we actually saw this. We live in amazing times, and I mean that in the worst way. But everything that happened in the first go-around of what we called the trade war, it was really nothing—it was a skirmish compared with what’s happening now. But now, the possibilities are huge.
There’s a whole field of economic research on what the field calls rent-seeking. Economies where the way to succeed in business is not to be good at business, but to be good at cultivating political connections. And much of that actually was about tariffs and import quotas, but typically in developing countries. So there was a large concern that in places like Brazil or India, they were actually sacrificing a lot of potential gainful economic activity because businesses were focused instead on currying political favor. Well, could that happen here? Yes, it could. Very much down the road. I mean, I have to say that the speed and scale of the stuff that’s going on makes me think that we may have a global trade war and massive disruption before we even get around to the cronyism. But it’s down there, it’s in there. It’s in the mix.
Elizabeth:
We have seen, before yesterday, a real stop-start, put-on put-off, someone complains and we delay for a month. So I think we’ll really have to see, post-yesterday, where this goes. And this is a helpful roadmap for what to look for.
Paul:
And we should bear in mind also that the rest of the world has agency too. And part of the issue here is that the chaotic nature of the rollout is—again, the rest of the world has agency. And if you want to avoid getting into a lot of tit-for-tat, you probably want to at least explain what you’re doing and not be offending other countries unnecessarily. But, of course, we are doing that. I mean, to make Canada turn anti-American really takes—I didn’t think that—that wasn’t on my dance card for my career.
Elizabeth:
Roosevelt has argued for a long time for the strategic and targeted use of tariffs alongside industrial policy. And also, of course, alongside a strong sense of what rules and regulations you have to use to control unproductive uses of corporate and market power in that context, to make sure that the incentive structure that you’re creating actually targets the gains that you’re trying to make. But we’ve also argued for a way to transition into those things that takes account of some of the concerns that you’ve raised in terms of creating a stable business environment for investment, creating predictability, explaining things to mitigate the risk of fallout. And we’ve heard members of the administration say, “hey, yes.” [They] admit that this is going to be a little bit painful for a while, but it’ll be beneficial in the end.
You started to say this, but can you just pick apart for us when we hear someone say, “there might be a little bit of turmoil for a while,” what are the real costs of what that kind of turmoil might be for businesses, workers, consumers?
Paul:
I actually don’t buy—I mean, yes, there’s short-term pain, but it’s not short-term pain in exchange for a long-run gain, by any economic model I can think of applying. It’s actually short-term pain in return for probably even bigger long-term pain. The story about how this gets better is really not there.
I’m not a purist free trader. I’m not a laissez-faire guy. I mean, there’s a kind of idealized version of the post–New Deal consensus, which is, leave economic activity up to the markets, and then we’ll have a social safety net. But that has never been enough. We always need some additional stuff. We always need some industrial policy. And I think we need it more than we have actually had. But the reality is that you still want to have a lot of [trade]. International trade has, for the most part, been a plus for the US economy. There were distributional issues, but even there, it’s probably been a net-plus for the great majority of workers. And you’d want to mitigate the parts that aren’t. So the idea that shutting it down is going to produce a better outcome 5, 10 years down the pike, there’s really no clear argument to that effect. What is true is that we have this additional overlay, which is that nobody knows what the world is gonna look like next year. And so this is a tremendous inhibiting force.
Normally, when people say that, well, protectionism causes recessions, my answer has been no. There are lots of reasons not to like protectionism, but there’s no story about how it causes recessions. But protectionism where nobody knows what it’s gonna be, where nobody knows what the tariff rates are gonna be next year, that could cause a recession. So we may have the first real tariff-induced recession that I’m aware of in history, like, now.
Elizabeth:
That will give us something to keep an eye on over the next year and more.
I’m gonna change topics a little bit. We started, a little bit, to talk about power in the economy. Who has it? Who doesn’t? It’s something that you’ve explored. In your book Conscience of a Liberal, you wrote something that I really like: “The New Deal did more than create a middle-class society. It also brought America closer to its democratic ideals by giving working Americans real political power and ending the dominant position of the wealthy elite.”
Particularly in the environment we’re in today, what do you think policymakers should be thinking about in terms of what we can do to bring that New Deal power lens both to this moment and to a moment where we would have the ability to set the rules to put our country on a better course?
Paul:
There are two ends to that. One is just giving ordinary working- or middle-class people effective vehicles to exert political influence. And of course, we have the vote. (There may be that there’s no “of course” about that, but in principle, at least we have votes.) But I don’t think we really realized how much a strong union movement contributed toward making democracy work better. You can say, well, why isn’t the individual right to vote enough? And the answer is, look, there’s collective action problems. Politics is completely pervasive of things that would be good if everybody did them, but maybe [there’s] no individual incentives. So organizing politically is always hard, and unions are a big force in that—or were. And to some extent, still are, but much less than they used to be. And that’s really important. We are a less democratic country in practice because we don’t have workers organized. That’s one end of it, and there may be other ways, although I have to admit that I’m not all that creative. I think the success of unions in really making America more American in the postwar generation is something that we have never managed to find other routes to do.
Then on the other hand, there’s the question of the influence of malefactors of great wealth. The influence of vast wealth. And you don’t have to get too much into current events to say, well, we can really see that. I have to say, going back now, it looks like the plutocrats of the Gilded Age, by contemporary standards, were remarkable in their restraint and discretion. They didn’t try to buy influence as openly as the plutocrats today do. So now there are things you can do. It’s funny that our great grandfathers were much more open than we are in saying that one of the purposes of progressive taxation is to actually limit extreme wealth. And not simply because it’s more money to serve the common people, but because extreme wealth distorts democracy. Woodrow Wilson was much more willing to say things that would be regarded as extremely radical leftism now.
So really to reclaim who we are as a nation, [who we] are supposed to be, we need to work on both those ends. We need to try to empower basically working Americans, ordinary workers to have a role. And maybe there are other things besides unions, but that’s the obvious route.
And then you also need to try both with rules about money and politics, but also perhaps, if we can eventually, [through] constraining policy that limits the accumulation of enormous fortunes. That also limits that distortion because we really are in a situation now where it’s—all of the warnings about, as FDR would have said, the powers of organized money seem far more acute now than they ever did in the past.
Elizabeth:
You mentioned ideas that once were acceptable to say in polite company that seem more radical now. This is sort of the business of Roosevelt, to think big about how we can solve these questions of the maldistribution of power in the economy and do them at a structural level. And how to make ideas about that part of the common sense. You’ve talked about how that is part of what happened with the New Deal—that New Deal institutions that were at first considered novel and radical, by the Eisenhower presidency had become [a] normal part of American life. How did that happen in your view, that change in the common sense? And what made them so enduring and what lessons can we find for today about how to reorient what seems impossible and what seems a normal part of life?
Paul:
One of the things that strikes me when I look at history, both of economic institutions and of economic ideas, is that lots of things seem radical and scary until people have had a chance to experience them. So there’s the famous Nancy Pelosi quote—often out of context—where she said that for people to really understand the Affordable Care Act, we have to pass it. And it wasn’t like we were going to pull one over on people. It was that, as long as it was merely a theoretical thing, as long as it was something in prospect, it was possible to tell scare stories about death panels and just say, what will this do? But then after a few years, it becomes part of the fabric of life. And then, by the time we actually came fairly close to losing it, people were outraged because even imperfect as it is, Obamacare is a terrifically important safety net for many people.
You see that on a much larger scale [with] the New Deal changes. So if you go back to when FDR did his really stem-winding address in 1936 about the “I welcome their hatred” thing. The thing that was really the flash point—[that] was widely portrayed on one side of the political spectrum as an outrageous step that would destroy the market economy—was actually not Social Security, but unemployment insurance. It was like, “oh my god. You’re gonna actually pay people when they don’t have jobs.” And it turned out that hey, that’s okay. In fact—unemployment insurance was the most important thing that got us through COVID with minimal hardship. And now there are people, there’s always people who want to do away with these safety net programs. But things that can be made to sound ominous and radical when no one has actually experienced them can, after a few years, become part of the landscape.
The New Deal first got us through the Great Depression, then got us through the war. And by the time the war was over, we had become a very different country—and I would say a much better country—in which people accepted that, yeah, we have a kind of public responsibility to limit extreme inequality, to limit extreme hardship.
Elizabeth:
I want to close this out with a note that you struck in your final New York Timescolumn last December. It was a tough one. You wrote, “optimism has been replaced by anger and resentment,” and that “the public no longer has faith that the people running things know what they’re doing, or that we can assume that they’re being honest.”
I think that applies to government. It also applies to a lot of institutions across the board. So here is my question for you: What do you think it will take to rebuild trust in public institutions? And also, on a more personal level, how do you find the hope that we can make it there from here?
Paul:
Well, there’s nothing like actually doing good to build trust. If we can find our way past the current turmoil, I think that there’s an underlying reservoir of optimism still in America. And if we can get our way past this, all of these things that led us to this rather scary moment, then a few years of good governance can actually do wonders. I mean, I’m older than you are, and certainly older than a lot of the people I deal with, but I remember the 1990s. And although there are many imperfections and lots of things, it’s hard to remember just how positive people were feeling about America by the end of that decade. And that was thrown away through a variety of bad decisions. But still, it’s not that distant. It’s not that inconceivable.
And so I would think that the way forward is to get people in power who really do try to use it for good, get good programs, get good policy, get decent people. And there’s a lot of strengths in America. And this atmosphere of distrust and feeling that everyone is out to get you is self-serving. That will go away fairly quickly if it’s demonstrably not true.
Now personally, I’m terrified. I’m not giving up, but you can see a lot of the things that we read about in the history books about how societies go wrong are no longer abstract. We can see those emotions, we can see those forces out there. But the truth is that a better environment is actually—people become more generous, more positive when things are going okay. And we really don’t want to have a situation where [this] zero-sum, “I’ve got mine, I don’t want anybody else to get it” thinking is validated by experience. So, try to make things work is how we go from here.
Elizabeth:
I can tell you one of the things that gives me hope, Paul, is that in a moment where we are watching some institutions capitulate and fold in a way that is really disheartening, we also have some voices that are getting louder, not softer, and I think one of them is yours. So I wanna say how appreciative I know I am personally and how excited I know the [Roosevelt] Institute is generally to have you on as a senior fellow, in part because I really do think you are a voice out there that’s making sense of what’s happening. That’s helping us put into a context that we can understand the flood of news that we are experiencing. And, again, to demonstrate what it looks like to be a consistent voice with good analysis and moral clarity about what’s happening now, and also who we have been in the past and who we could be again. So we really appreciate your work, and we really appreciate you taking the time to chat today.
Healthcare is big business. That’s why JP Morgan Chase is hosting its 42nd Healthcare Conference in San Francisco starting today– the same week Congress reconvenes in DC with the business of healthcare on its agenda as well. The predispositions of the two toward the health industry could not be more different.
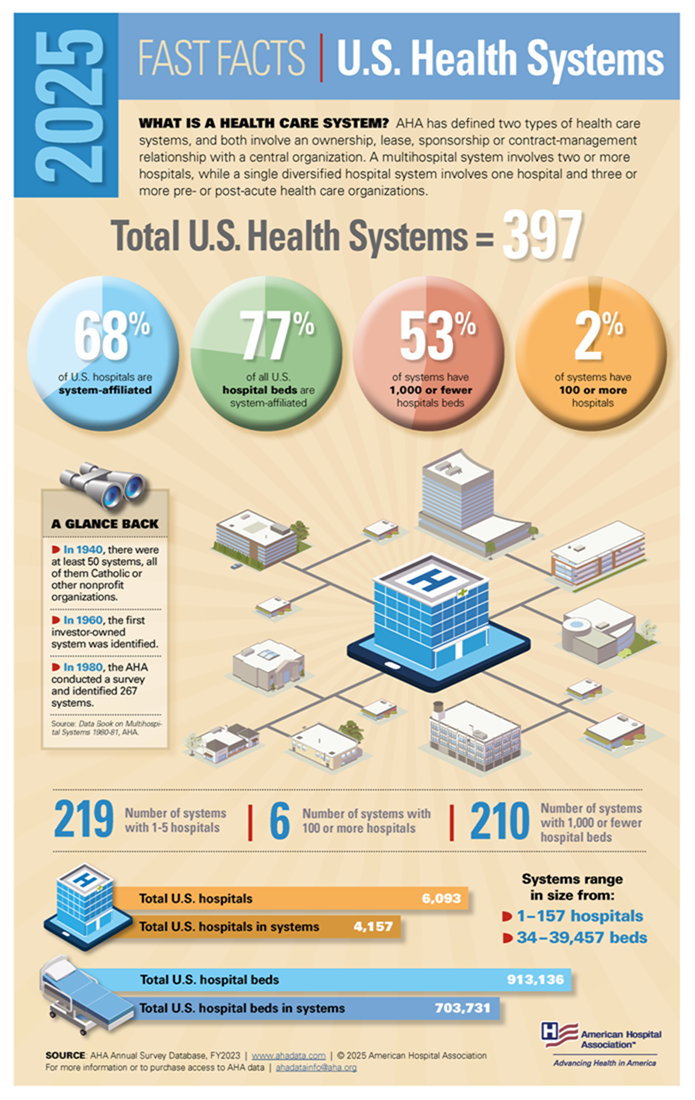
Context: the U.S. Health System in the Global Economy
Though the U.S. population is only 4% of the world total, our spending for healthcare products and services represents 45% of global healthcare market. Healthcare is 17.4% of U.S. GDP vs. an average of 9.6% for the economies in the 37 other high-income economies of the world. It is the U.S.’ biggest private employer (17.2 million) accounting for 24% of total U.S. job growth last year (BLS). And it’s a growth industry: annual health spending growth is forecast to exceed 4%/year for the foreseeable future and almost 5% globally—well above inflation and GDP growth. That’s why private investments in healthcare have averaged at least 15% of total private investing for 20+ years. That’s why the industry’s stability is central to the economy of the world.
The developed health systems of the world have much in common: each has three major sets of players:
Service Providers: organizations/entities that provide hands-on services to individuals in need (hospitals, physicians, long-term care facilities, public health programs/facilities, alternative health providers, clinics, et al). In developed systems of the world, 50-60% of spending is in these sectors.
Innovators: organizations/entities that develop products and services used by service providers to prevent/treat health problems: drug and device manufacturers, HIT, retail health, self-diagnostics, OTC products et al. In developed systems of the world, 20-30% is spend in these.
Administrators, Watchdogs & Regulators: Organizations that influence and establish regulations, oversee funding and adjudicate relationships between service providers and innovators that operate in their systems: elected officials including Congress, regulators, government agencies, trade groups, think tanks et al. In the developed systems of the world, administration, which includes insurance, involves 5-10% of its spending (though it is close to 20% in the U.S. system due to the fragmentation of our insurance programs).
In the developed systems of the world, including the U.S., the role individual consumers play is secondary to the roles health professionals play in diagnosing and treating health problems. Governments (provincial/federal) play bigger roles in budgeting and funding their systems and consumer out-of-pocket spending as a percentage of total health spending is higher than the U.S. All developed and developing health systems of the world include similar sectors and all vary in how their governments regulate interactions between them. All fund their systems through a combination of taxes and out-of-pocket payments by consumers. All depend on private capital to fund innovators and some service providers. And all are heavily regulated.
In essence, that makes the U.S. system unique are (1) the higher unit costs and prices for prescription drugs and specialty services, (2) higher administrative overhead costs, (3) higher prevalence of social health issues involving substance abuse, mental health, gun violence, obesity, et al (4) the lack of integration of our social services/public health and health delivery in communities and (5) lack of a central planning process linked to caps on spending, standardization of care based on evidence et al.
So, despite difference in structure and spending, developed systems of the world, like the U.S. look similar:
The Current Climate for the U.S. Health Industry
The global market for healthcare is attractive to investors and innovators; it is less attractive to most service providers since their business models are less scalable. Both innovator and service provider sectors require capital to expand and grow but their sources vary: innovators are primarily funded by private investors vs. service providers who depend more on public funding. Both are impacted by the monetary policies, laws and political realities in the markets where they operate and both are pivoting to post-pandemic new normalcy. But the outlook of investors in the current climate is dramatically different than the predisposition of the U.S. Congress toward healthcare:
Healthcare innovators and their investors are cautiously optimistic about the future. The dramatic turnaround in the biotech market in 4Q last year coupled with investor enthusiasm for generative AI and weight loss drugs and lower interest rates for debt buoy optimism about prospects at home and abroad. The FDA approved 57 new drugs last year—the most since 2018. Big tech is partnering with established payers and providers to democratize science, enable self-care and increase therapeutic efficacy. That’s why innovators garner the lion’s share of attention at JPM. Their strategies are longer-term focused: affordability, generative AI, cost-reduction, alternative channels, self-care et al are central themes and the welcoming roles of disruptors hardwired in investment bets. That’s the JPM climate in San Franciso.
By contrast, service providers, especially the hospital and long-term care sectors, are worried. In DC, Congress is focused on low-hanging fruit where bipartisan support is strongest and political risks lowest i.e.: price transparency, funding cuts, waste reduction, consumer protections, heightened scrutiny of fraud and (thru the FTC and DOJ) constraints on horizontal consolidation to protect competition. And Congress’ efforts to rein in private equity investments to protect consumer choice wins votes and worries investors. Thus, strategies in most service provider sectors are defensive and transactional; longer-term bets are dependent on partnerships with private equity and corporate partners. That’s the crowd trying to change Congress’ mind about cuts and constraints.
The big question facing JPM attendees this week and in Congress over the next few months is the same: is the U.S. healthcare system status quo sustainable given the needs in other areas at home and abroad?
Investors and organizations at JPM think the answer is no and are making bets with their money on “better, faster, cheaper” at home and abroad. Congress agrees, but the political risks associated with transformative changes at home are too many and too complex for their majority.
For healthcare investors and operators, the distance between San Fran and DC is further and more treacherous than the 2808 miles on the map.
The JPM crowd sees a global healthcare future that welcomes change and needs capital; Congress sees a domestic money pit that’s too dicey to handle head-on–two views that are wildly divergent.
Last week was notable for healthcare because current events thrust it into the limelight…
Hospitals and emergency responders in Maine: Media attention to Gaza and the Speaker-less U.S. House of Representatives was temporarily suspended as the deaths of 18 in the U.S.’ 36h mass shooting in Lewiston, Maine took center stage. The immediate overload on Lewiston’s Central Maine Medical Center and Mass General where the 13 injured were treated (including 4 still hospitalized) drew media attention—largely gone by Friday when the shooter’s death by suicide was confirmed.
The New Speaker of the House: The GOP House of Representatives elected Mike Johnson, the 4-term Representative from Shreveport to the post vacant since October 3.
Johnson is no stranger to partisan positions on healthcare issues. As Chairman of the conservative-leaning Republican Steering Committee from 2019-2021, he led the group’s platform to dismantle the Affordable Care Act and supports a national restriction on abortions despite Senate GOP Leader McConnell’s preference it be left to states to decide.
With the prospect of a government shutdown November 17 due to inaction on the FY2024 federal budget, the 52-year-old lawyer faces delicate maneuvering around $106 billion proposed for Israel, the Ukraine, Taiwan and border security alongside appropriations for the health system that consumes 28% of entire federal outlays.
Health organizational business strategy announcements: Friction between physicians and hospital officials in Asheville (Mission) and Minnesota (Allina) attracted national coverage and brought attention to staffing, cultural and financial circumstances in these prominent organizations. —and on the heels of the Kaiser Permanente strike settlement. The divorce from Mass General by Dana Farber in Boston and announcements by GNC, Best Buy, Optum (re-branding NaviHealth) and Sanofi hit last week’s news cycle.
And indirectly, the 3Q 2023 GDP report by the Department of Commerce raised eyebrows: it was up 4.9%–far higher than expected prompting speculation that the Federal Open Market Committee (FOMC) will raise interest rates (again) at its meeting this week or next month. That means borrowing costs for struggling hospitals, nursing homes and consumers needing loans will go up along with household medical debt.
As news cycles go, this one was standard fare for healthcare: with the exception of business plan announcements by organizations or as elements of tragedies like Lewiston, Gaza or a pandemic,
the business of the health system—how it operates is largely uncovered and often subject to misinformation or disinformation.
That’s the problem: it’s background noise to most voters who can be stoked to action over a single issue when prompted by special interests (i.e., Abortion rights, surprise billing, price transparency et al) but remain inattentive and marginally informed about the bigger role it plays in our communities and country and where it’s heading long-term.
The narrative common to most boils down to these:
The U.S. health system is good, but it’s complicated. ‘How good’ depends on your insurance and your health—both are key.
The U.S. health system is expensive and profitable. It pays its executives well and its frontline workers unfairly.
The delivery system focuses on the sick and injured; prevention and public health matter less.
Hospitals and physicians are vital to the system; health insurers keep their costs down.
The U.S. system pays lip service to “customer service” and ‘engaged consumers.” It is spin not supported by actions.
The U.S. system needs to change dramatically.
In the next 3 weeks, attention will be on the federal budget: healthcare will be in the background unless temporarily an element of a mass tragedy. Each trade group will tout its accomplishments to regulators and pimp their advocacy punch list. Each company will gin-out news releases and commentary about the future of the system will default to think tanks and focused on a single issue of interest.
That’s the problem. In this era of social media, polarization, and mass transparency, these old ways of communicating no longer work. Left unattended, they undermine the value proposition on which the U.S. system is based.
Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
An argument for humility in the face of pandemic forecasting unknown unknowns.
“Are we battling an unprecedented pandemic or panicking at a computer generated mirage?” I asked at the beginning of the COVID-19 pandemic on March 18, 2020. Back then the Imperial College London epidemiological model’s baseline scenario projected that with no changes in individual behaviors and no public health interventions, more than 80 percent of Americans would eventually be infected with novel coronavirus and about 2.2 million would die of the disease. This implies that 0.8 percent of those infected would die of the disease. This is about 8-times worse than the mortality rate from seasonal flu outbreaks.
Spooked by these dire projections, President Donald Trump issued on March 16 his Coronavirus Guidelines for America that urged Americans to “listen to and follow the directions of STATE AND LOCAL AUTHORITIES.” Among other things, Trump’s guidelines pressed people to “work or engage in schooling FROM HOME whenever possible” and “AVOID SOCIAL GATHERINGS in groups of more than 10 people.” The guidelines exhorted Americans to “AVOID DISCRETIONARY TRAVEL, shopping trips and social visits,” and that “in states with evidence of community transmission, bars, restaurants, food courts, gyms, and other indoor and outdoor venues where people congregate should be closed.”
Let’s take a moment to recognize just how blindly through the early stages of the pandemic we—definitely including our public health officials—were all flying at the time. The guidelines advised people to frequently wash their hands, disinfect surfaces, and avoid touching their faces. Basically, these were the sort of precautions typically recommended for influenza outbreaks. On July 9, 2020, an open letter from 239 researchers begged the World Health Organization and other public health authorities to recognize that COVID-19 was chiefly spread by airborne transmission rather than via droplets deposited on surfaces. The U.S. Centers for Disease Control and Prevention (CDC) didn’t update its guidance on COVID-19 airborne transmission until May 2021. And it turns out that touching surfaces is not a major mode of transmission for COVID-19.
The president’s guidelines also advised, “IF YOU FEEL SICK, stay home. Do not go to work.” This sensible advice, however, missed the fact that a huge proportion of COVID-19 viral transmission occurred from people without symptoms. That is, people who feel fine can still be infected and, unsuspectingly, pass along their virus to others. For example, one January 2021 study estimated that “59% of all transmission came from asymptomatic transmission, comprising 35% from presymptomatic individuals and 24% from individuals who never develop symptoms.”
The Imperial College London’s alarming projections did not go uncontested. A group of researchers led by Stanford University medical professor Jay Bhattacharya believed that COVID-19 infections were much more widespread than the reported cases indicated. If the Imperial College London’s hypothesis were true, Bhattacharya and his fellow researchers argued, that would mean that the mortality rate and projected deaths from the coronavirus would be much lower, making the pandemic much less menacing.
The researchers’ strategy was to blood test people in Santa Clara and Los Angeles Counties in California to see how many had already developed antibodies in response to coronavirus infections. Using those data, they then extrapolated what proportion of county residents had already been exposed to and recovered from the virus.
Bhattacharya and his colleagues preliminarily estimated that between 48,000 and 81,000 people had already been infected in Santa Clara County by early April, which would mean that COVID-19 infections were “50-85-fold more than the number of confirmed cases.” Based on these data the researchers calculated that toward the end of April “a hundred deaths out of 48,000-81,000 infections corresponds to an infection fatality rate of 0.12-0.2%.” As I optimistically reported at the time, that would imply that COVID-19’s lethality was not much different than for seasonal influenza.
Bhattacharya and his colleagues conducted a similar antibody survey in Los Angeles County. That study similarly asserted that COVID-19 infections were much more widespread than reported cases. The study estimated 2.8 to 5.6 percent of the residents of Los Angeles County had been infected by early April. That translates to approximately 221,000 to 442,000 adults in the county who have had the infection. “That estimate is 28 to 55 times higher than the 7,994 confirmed cases of COVID-19 reported to the county by the time of the study in early April,” noted the accompanying press release. “The number of COVID-related deaths in the county has now surpassed 600.” These estimates would imply a relatively low infection fatality rate of between 0.14 and 0.27 percent.
Unfortunately, from the vantage of 14 months, those hopeful results have not been borne out. Santa Clara County public health officials report that there have been 119,712 diagnosed cases of COVID-19 so far. If infections were really being underreported by 50-fold, that would suggest that roughly 6 million Santa Clara residents would by now have been infected by the coronavirus. The population of the county is just under 2 million. Alternatively, extrapolating a 50-fold undercount would imply that when 40,000 diagnosed cases were reported on July 11, 2020, all 2 million people living in Santa Clara County had been infected by that date.
Los Angeles County reports 1,247,742 diagnosed COVID-19 cases cumulatively. Again, if infections were really being underreported 28-fold, that would imply that roughly 35 million Angelenos out of a population of just over 10 million would have been infected with the virus by now. Again turning the 28-fold estimate on its head, that would imply that all 10 million Angelenos would have been infected when 360,000 cases had been diagnosed on November 21, 2020.
COVID-19 cases are, of course, being undercounted. Data scientist Youyang Gu has been consistently more accurate than many of the other researchers parsing COVID-19 pandemic trends. Gu estimates that over the course of the pandemic, U.S. COVID-19 infections have roughly been 4-fold greater than diagnosed cases. Applying that factor to the number of reported COVID-19 cases would yield an estimate of 480,000 and 5,000,000 total infections in Santa Clara and Los Angeles respectively. If those are ballpark accurate, that would mean that the COVID-19 infection fatality rate in Santa Clara is 0.46 percent and is 0.49 percent in Los Angeles. Again, applying a 4-fold multiplier to take account of undercounted infections, those are both just about where the U.S. infection fatality rate of 0.45 percent is now.
The upshot is that, so far, we have ended up about half-way between the best case and worst case scenarios sketched out at the beginning of the pandemic.
One hesitates to elevate obviously bad arguments, even to point out how bad they are. This is a conundrum that comes up a lot these days, as members of the media measure the utility of reporting on bad faith, disingenuous or simply bizarre claims.
If someone were to insist, for example, that they were not going to get the coronavirus vaccine solely to spite the political left, should that claim be elevated? Can we simply point out how deranged it is to refuse a vaccine that will almost certainly end an international pandemic simply because people with whom you disagree think that maybe this is a good route to end that pandemic? If someone were to write such a thing at some attention-thirsty website, we certainly wouldn’t want to link to it, leaving our own readers having to figure out where it might be found should they choose to do so.
In this case, it’s worth elevating this argument (which, to be clear, is actually floating out there) to point out one of the myriad ways in which the effort to vaccinate as many adults as possible has become interlaced with partisan politics. As the weeks pass and demand for the vaccine has tapered off, the gap between Democratic and Republican interest in being vaccinated seems to be widening — meaning that the end to the pandemic is likely to move that much further into the future.
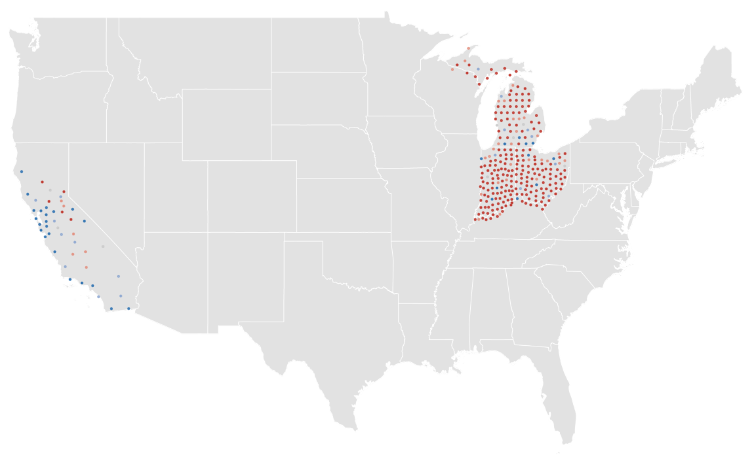
Consider, for example, the rate of completed vaccinations by county, according to data compiled by CovidActNow. You can see a slight correlation between how a county voted in 2020 — the horizontal axis — and the density of completed vaccinations, shown on the vertical. There’s a greater density of completed vaccinations on the left side of the graph than on the right.
If we shift to the percentage of the population that’s received even one dose of the vaccine, the effect is much more obvious.
This is a relatively recent development. At the beginning of the month, the density of the population that had received only one dose resulted in a graph that looked much like the current density of completed doses.
If we animate those two graphs, the effect is obvious. In the past few weeks, the density of first doses has increased much faster in more-Democratic counties.
If we group the results of the 2020 presidential contest into 20-point buckets, the pattern is again obvious.
It’s not a new observation that Republicans are less willing to get the vaccine; we’ve reported on it repeatedly. What’s relatively new is how that hesitance is showing up in the actual vaccination data.
A Post-ABC News poll released on Monday showed that this response to the vaccine holds even when considering age groups. We’ve known for a while that older Americans, who are more at risk from the virus, have been more likely to seek the vaccine. But even among seniors, Republicans are significantly more hesitant to receive the vaccine than are Democrats.
This is a particularly dangerous example of partisanship. People 65 or older have made up 14 percent of coronavirus infections, according to federal data, but 81 percent of deaths. That’s among those for whom ages are known, a subset (though a large majority) of overall cases. While about 1.8 percent of that overall group has died, the figure for those aged 65 and over is above 10 percent.
As vaccines have been rolled out across the country, you can see how more-heavily-blue counties have a higher density of vaccinations in many states.
This is not a universal truth, of course. Some heavily Republican counties have above-average vaccination rates. (About 40 percent of counties that preferred former president Donald Trump last year are above the average in the CovidActNow data. The rate among Democratic counties is closer to 80 percent.) But it is the case that there is a correlation between how a county voted and how many of its residents have been vaccinated. It is also the case that the gap between red and blue counties is widening.
Given all of that, it probably makes sense to point out that an argument against vaccines based on nothing more than “lol libs will hate this” is an embarrassing argument to make.











{kind=link}