

Cartoon – Doctor’s Advice
Click to access CBC_72_08052020_Final.pdf
[Readers’ Note: This is the first of two articles on the Future of Hospitals in Post-COVID America. This article
examines how market forces are consolidating, rationalizing and redistributing acute care assets within the
broader industry movement to value-based care delivery. The second article, which will publish next month,
examines gaps in care delivery and the related public policy challenges of providing appropriate, accessible
and affordable healthcare services in medically-underserved communities.]
In her insightful 2016 book, The Gray Rhino: How to Recognize and Act on the Obvious Dangers We Ignore,
Michelle Wucker coins the term “Gray Rhinos” and contrasts them with “Black Swans.” That distinction is
highly relevant to the future of American hospitals.
Black Swans are high impact events that are highly improbable and difficult to predict. By contrast, Gray
Rhinos are foreseeable, high-impact events that we choose to ignore because they’re complex, inconvenient
and/or fortified by perverse incentives that encourage the status quo. Climate change is a powerful example
of a charging Gray Rhino.
In U.S. healthcare, we are now seeing what happens when a Gray Rhino and a Black Swan collide.
Arguably, the nation’s public health defenses should anticipate global pandemics and apply resources
systematically to limit disease spread. This did not happen with the coronavirus pandemic.
Instead, COVID-19 hit the public healthcare infrastructure suddenly and hard. This forced hospitals and health systems to dramatically reduce elective surgeries, lay off thousands and significantly change care delivery with the adoption of new practices and services like telemedicine.
In comparison, many see the current American hospital business model as a Gray Rhino that has been charging toward
unsustainability for years with ever-building momentum.
Even with massive and increasing revenue flows, hospitals have long struggled with razor-thin margins, stagnant payment rates and costly technology adoptions. Changing utilization patterns, new and disruptive competitors, pro-market regulatory rules and consumerism make their traditional business models increasingly vulnerable and, perhaps, unsustainable.
Despite this intensifying pressure, many hospitals and health systems maintain business-as-usual practices because transformation is so difficult and costly. COVID-19 has made the imperative of change harder to ignore or delay addressing.
For a decade, the transition to value-based care has dominated debate within U.S. healthcare and absorbed massive strategic,
operational and financial resources with little progress toward improved care outcomes, lower costs and better customer service. The hospital-based delivery system remains largely oriented around Fee-for-Service reimbursement.
Hospitals’ collective response to COVID-19, driven by practical necessity and financial survival, may accelerate the shift to value-based care delivery. Time will tell.
This series explores the repositioning of hospitals during the next five years as the industry rationalizes an excess supply of acute care capacity and adapts to greater societal demands for more appropriate, accessible and affordable healthcare services.
It starts by exploring the role of the marketplace in driving hospital consolidation and the compelling need to transition to value-based care delivery and payment models.
COVID’s DUAL SHOCKS TO PATIENT VOLUME
Many American hospitals faced severe financial and operational challenges before COVID-19. The sector has struggled to manage ballooning costs, declining margins and waves of policy changes. A record 18 rural hospitals closed in 2019. Overall, hospitals saw a 21% decline in operating margins in 2018-2019.
COVID intensified those challenges by administering two shocks to the system that decreased the volume of hospital-based activities and decimated operating margins.
The first shock was immediate. To prepare for potential surges in COVID care, hospitals emptied beds and cancelled most clinic visits, outpatient treatments and elective surgeries. Simultaneously, they incurred heavy costs for COVID-related equipment (e.g. ventilators,PPE) and staffing. Overall, the sector experienced over $200 billion in financial losses between March and June 20204.
The second, extended shock has been a decrease in needed but not necessary care. Initially, many patients delayed seeking necessary care because of perceived infection risk. For example, Emergency Department visits declined 42% during the early phase of the pandemic.
Increasingly, patients are also delaying care because of affordability concerns and/or the loss of health insurance. Already, 5.4 million people have lost their employer-sponsored health insurance. This will reduce incremental revenues associated with higher-paying commercial insurance claims across the industry. Additionally, avoided care reduces patient volumes and hospital revenues today even as it increases the risk and cost of future acute illness.
The infusion of emergency funding through the CARES Act helped offset some operating losses but it’s unclear when and even whether utilization patterns and revenues will return to normal pre-COVID levels. Shifts in consumer behavior, reductions in insurance coverage, and the emergence of new competitors ranging from Walmart to enhanced primary care providers will likely challenge the sector for years to come.
The disruption of COVID-19 will serve as a forcing function, driving meaningful changes to traditional hospital business models and the competitive landscape. Frankly, this is long past due. Since 1965, Fee-for-Service (FFS) payment has dominated U.S. healthcare and created pervasive economic incentives that can serve to discourage provider responsiveness in transitioning to value-based care delivery, even when aligned to market demand.
Telemedicine typifies this phenomenon. Before COVID, CMS and most health insurers paid very low rates for virtual care visits or did not cover them at all. This discouraged adoption of an efficient, high-value care modality until COVID.
Unable to conduct in-person clinical visits, providers embraced virtual care visits and accelerated its mass adoption. CMS and
commercial health insurers did their part by paying for virtual care visits at rates equivalent to in-person clinic visits. Accelerated innovation in care delivery resulted.
THE COMPLICATED TRANSITION TO VALUE
Broadly speaking, health systems and physician groups that rely almost exclusively on activity-based payment revenues have struggled the most during this pandemic. Vertically integrated providers that offer health insurance and those receiving capitated payments in risk-based contracts have better withstood volume losses.
Modern Healthcare notes that while provider data is not yet available, organizations such as Virginia Care Partners, an integrated network and commercial ACO; Optum Health (with two-thirds of its revenue risk-based); and MediSys Health Network, a New Yorkbased NFP system with 148,000 capitated and 15,000 shared risk patients, are among those navigating the turbulence successfully. As the article observes,
…providers paid for value have had an easier time weathering the storm…. helped by a steady source of
income amid the chaos. Investments they made previously in care management, technology and social
determinants programs equipped them to pivot to new ways of providing care.
They were able to flip the switch on telehealth, use data and analytics to pinpoint patients at risk for
COVID-19 infection, and deploy care managers to meet the medical and nonclinical needs of patients even
when access to an office visit was limited.
Supporting this post-COVID push for value-based care delivery, six former leaders from CMS wrote to Congress in
June 2020 calling for providers, commercial insurers and states to expand their use of value-based payment models to
encourage stability and flexibility in care delivery.
If value-based payment models are the answer, however, adoption to date has been slow, limited and difficult. Ten
years after the Affordable Care Act, Fee-for-Service payment still dominates the payer landscape. The percentage of
overall provider revenue in risk-based capitated contracts has not exceeded 20%
Despite improvements in care quality and reductions in utilization rates, cost savings have been modest or negligible.
Accountable Care Organizations have only managed at best to save a “few percent of Medicare spending, [but] the
amount varies by program design.”
While most health systems accept some forms of risk-based payments, only 5% of providers expect to have a majority
(over 80%) of their patients in risk-based arrangements within 5 years.
The shift to value is challenging for numerous reasons. Commercial payers often have limited appetite or capacity for
risk-based contracting with providers. Concurrently, providers often have difficulty accessing the claims data they need
from payers to manage the care for targeted populations.
The current allocation of cost-savings between buyers (including government, employers and consumers), payers
(health insurance companies) and providers discourages the shift to value-based care delivery. Providers would
advance value-based models if they could capture a larger percentage of the savings generated from more effective
care management and delivery. Those financial benefits today flow disproportionately to buyers and payers.
This disconnection of payment from value creation slows industry transformation. Ultimately, U.S. healthcare will not
change the way it delivers care until it changes the way it pays for care. Fortunately, payment models are evolving to
incentivize value-based care delivery.
As payment reform unfolds, however, operational challenges pose significant challenges to hospitals and health
systems. They must adopt value-oriented new business models even as they continue to receive FFS payments. New
and old models of care delivery clash.
COVID makes this transition even more formidable as many health systems now lack the operating stamina and
balance sheet strength to make the financial, operational and cultural investments necessary to deliver better
outcomes, lower costs and enhanced customer service.
MARKET-DRIVEN CONSOLIDATION AND TRANSFORMATION
Full-risk payment models, such as bundled payments for episodic care and capitation for population health, are the
catalyst to value-based care delivery. Transition to value-based care occurs more easily in competitive markets with
many attributable lives, numerous provider options and the right mix of willing payers.
As increasing numbers of hospitals struggle financially, the larger and more profitable health systems are expanding
their networks, capabilities and service lines through acquisitions. This will increase their leverage with commercial
payers and give them more time to adapt to risk-based contracting and value-based care delivery.
COVID also will accelerate acquisition of physician practices. According to an April 2020 MGMA report, 97% of
physician practices have experienced a 55% decrease in revenue, forcing furloughs and layoffs15. It’s estimated the
sector could collectively lose as much as $15.1 billion in income by the end of September 2020.
Struggling health systems and physician groups that read the writing on the wall will pro-actively seek capital or
strategic partners that offer greater scale and operating stability. Aggregators can be selective in their acquisitions,
seeking providers that fuel growth, expand contiguous market positions and don’t dilute balance sheets.
Adding to the sector’s operating pressure, private equity, venture investors and payers are pouring record levels of
funding into asset-light and virtual delivery companies that are eager to take on risk, lower prices by routing procedures
and capture volume from traditional providers. With the right incentives, market-driven reforms will reallocate resources
to efficient companies that generate compelling value.
As this disruption continues to unfold, rural and marginal urban communities that lack robust market forces will
experience more facility and practice closures. Without government support to mitigate this trend, access and care gaps
that already riddle American healthcare will unfortunately increase.
WINNING AT VALUE
The average hospital generates around $11,000 per patient discharge. With ancillary services that can often add up to
more than $15,000 per average discharge. Success in a value-based system is predicated on reducing those
discharges and associated costs by managing acute care utilization more effectively for distinct populations (i.e.
attributed lives).
This changes the orientation of healthcare delivery toward appropriate and lower cost settings. It also places greater
emphasis on preventive, chronic and outpatient care as well as better patient engagement and care coordination.
Such a realignment of care delivery requires the following:
A tight primary care network (either owned or affiliated) to feed referrals and reduce overall costs through
better preventive care.
A gatekeeper or navigator function (increasingly technology-based) to manage / direct patients to the most
appropriate care settings and improve coordination, adherence and engagement.
A carefully designed post-acute care network (including nursing homes, rehab centers, home care
services and behavioral health services, either owned or sufficiently controlled) to manage the 70% of
total episode-of-care costs that can occur outside the hospital setting.
An IT infrastructure that can facilitate care coordination across all providers and settings.
Quality data and digital tools that enhance care, performance, payment and engagement.
Experience with managing risk-based contracts.
A flexible approach to care delivery that includes digital and telemedicine platforms as well as nontraditional sites of care.
Aligned or incentivized physicians.
Payer partners willing to share data and offload risk through upside and downside risk contracts.
Engaged consumers who act on their preferences and best interests.
While none of these strategies is new or controversial, assembling them into cohesive and scalable business models is
something few health systems have accomplished. It requires appropriate market conditions, deep financial resources,
sophisticated business acumen, operational agility, broad stakeholder alignment, compelling vision, and robust
branding.
Providers that fail to embrace value-based care for their “attributed lives” risk losing market relevance. In their relentless pursuit of increasing treatment volumes and associated revenues, they will lose market share to organizations that
deliver consistent and high-value care outcomes.
CONCLUSION: THE CHARGING GRAY RHINO
America needs its hospitals to operate optimally in normal times, flex to manage surge capacity, sustain themselves
when demand falls, create adequate access and enhance overall quality while lowering total costs. That is a tall order
requiring realignment, evolution, and a balance between market and policy reform measures.
The status quo likely wasn’t sustainable before COVID. The nation has invested heavily for many decades in acute and
specialty care services while underinvesting, on a relative basis, in primary and chronic care services. It has excess
capacity in some markets, and insufficient access in others.
COVID has exposed deep flaws in the activity-based payment as well as the nation’s underinvestment in public health.
Disadvantaged communities have suffered disproportionately. Meanwhile, the costs for delivering healthcare services
consume an ever-larger share of national GDP.
Transformational change is hard for incumbent organizations. Every industry, from computer and auto manufacturing to
retailing and airline transportation, confronts gray rhino challenges. Many companies fail to adapt despite clear signals
that long-term viability is under threat. Often, new, nimble competitors emerge and thrive because they avoid the
inherent contradictions and service gaps embedded within legacy business models.
The healthcare industry has been actively engaged in value-driven care transformation for over ten years with little to
show for the reform effort. It is becoming clear that many hospitals and health systems lack the capacity to operate
profitably in competitive, risk-based market environments.
This dismal reality is driving hospital market valuations and closures. In contrast, customers and capital are flowing to
new, alternative care providers, such as OneMedical, Oak Street Health and Village MD. Each of these upstart
companies now have valuations in the $ billions. The market rewards innovation that delivers value.
Unfortunately, pure market-driven reforms often neglect a significant and growing portion of America’s people. This gap has been more apparent as COVID exacts a disproportionate toll on communities challenged by higher population
density, higher unemployment, and fewer medical care options (including inferior primary and preventive care infrastructure).
Absent fundamental change in our hospitals and health systems, and investment in more efficient care delivery and
payment models, the nation’s post-COVID healthcare infrastructure is likely to deteriorate in many American
communities, making them more vulnerable to chronic disease, pandemics and the vicissitudes of life.
Article 2 in our “Future of Hospitals” series will explore the public policy challenges of providing appropriate, affordable and accessible healthcare to all American communities.

Four months into the COVID-19 pandemic, fewer than 10% of U.S. primary care practices have been able to stabilize operations.
Nearly 9 in 10 primary care practices continue to face significant difficulties with COVID-19, including obtaining medical supplies, meeting the increasing health needs of their patients, and finding sufficient resources to remain operational, according to a recent survey of close to 600 primary care clinicians in 46 states.
Only 13% of primary care clinicians say they are adapting to a “new normal” in the protracted pandemic, the survey found.
More than four months into the pandemic and at a time when 39 states are experiencing an increase of COVID-19 cases, fewer than 4 in 10 clinicians feel confident and safe with their access to personal protective equipment, according to the survey from the Larry A. Green Center in partnership with the Primary Care Collaborative, which was conducted July 10 to July 13.
Among the primary care clinicians surveyed, 11% report that staff in their practice have quit in the last four weeks over safety concerns.
A primary care provider in Ohio said this: “The ‘I can do 4-6 weeks of this’ transition to ‘this feels like a new/permanent normal’ is crushing and demoralizing. Ways to build morale when everyone is at a computer workstation away from other staff (and patients) feels impossible.”
“In the first few months of the pandemic, the country pulled together to stop the spread of the virus, and it seemed like we were making progress. Primary care clinicians and practices were working hard, against tremendous challenges,” said Rebecca Etz, Ph.D., co-director of The Larry A. Green Center in a statement.
“But now the country is backsliding, and it’s clear that primary care doesn’t have enough strength to deal with the rising number of cases. If primary care were a COVID-19 patient, it would be flat on its back,” Etz said.
The survey conducted by the Larry A. Green Center is part of an ongoing series looking at the attitudes of primary care clinicians and patients during the COVID-19 pandemic and the abilities of practices to meet patients’ needs.
Close to 40% of primary care providers report they are maxed out with mental exhaustion and 18% say they spend each week wondering if their practice or job will still be there next week.
In addition to feeling stressed, clinicians and their practices are also experiencing upheaval. The survey found that 22% of clinicians report skipped or deferred salaries, and 78% report preventive and chronic care is being deferred or delayed by patients.
Primary care clinicians report that 42% of in-person volume is down but overall contact with patients is high, while 39% report not being able to bill for the majority of work delivered, the survey found.
“Given the rapidly rising infection rates and persistent lack of PPE, more than a third of primary care clinicians are reporting feeling unsafe at the office, and 20% are cutting back on face-to-face visits while doing more remote outreach,” said Ann Greiner, president and CEO of the Primary Care Collaborative in a statement.
Greiner said this is a clear signal that payers must advance or retain parity for telehealth and telephonic calls.
“It also is a clarion call to move to a new payment system that doesn’t rely on face-to-face visits and that is prospective so practices can better manage patient care,” she said.
Providers say they need more support from private insurers, particularly when it comes to reimbursing for telehealth and telephone visits.
According to the survey, a primary care doctor in Illinois said, “Recently told we would not be able to conduct telephone visits due to lack of reimbursement. I work in a low-income Medicare population which has low health literacy and no technology literacy. We were 80% telephone and 20% Zoom and in-office. This further exemplifies the extreme health care disparities in the U.S.”
https://abc7.com/new-kaiser-school-pasadena-bernard-j-tyson-of-medicine-permanente-medical/6336881/
![New Kaiser Permanente medical school set to open in Pasadena [Video]](https://s.yimg.com/uu/api/res/1.2/IfF3Q6Q1OF1Bq9CP_D.mZg--~B/aD03MjA7dz0xMjgwO3NtPTE7YXBwaWQ9eXRhY2h5b24-/https://s.yimg.com/hd/cp-video-transcode/prod/2020-07/27/5f1f0541fd04d4312d059439/5f1f0541fd04d4312d05943a_o_U_v2.jpg)
The new Kaiser Permanente medical school in Pasadena opened its doors to faculty and students for the first time Monday, with free tuition through 2024.
The Bernard J. Tyson School of Medicine opened for its inaugural class of 50 students in the midst of the coronavirus pandemic, which officials say presents “unparalleled challenges.”
The pandemic has forced the school to make adjustments, including adopting a “hybrid model” that includes in-class and virtual programs and more frequent cleaning, Walter Harris, the school’s senior vice president of administration and finance, told City News Service. He said some classes could be held with some students in one classroom and others watching from another classroom via Zoom.
The school has waived tuition, fees and disability insurance for students entering through the fall of 2024, and students in those classes will receive a waiver for the cost of a health plan from Kaiser Permanente unless they have an equivalent health plan, according to the school’s website.
The four-story, state-of-the-art building could accommodate twice as many students, which easily enables physical distancing, Harris said.
Students have been advised they need to wear face masks, and the school will have plenty of hand sanitizer and wipes available, he added.
None of the students objected to the school opening as scheduled, according to Harris, who said they are “very excited to get their medical careers started.”
The school includes an anatomy resource center in which traditional cadaver dissection will be replaced with newer methods that are more clinically relevant, along with a rooftop garden with a meditation, yoga and fitness area for student and faculty “wellness.”
Students are set to begin interacting with patients during their third week of school and to learn from Kaiser Permanente physicians and care teams at six of its medical center campuses, including Los Angeles, West L.A. and Downey.
https://khn.org/news/dental-and-doctors-offices-still-struggling-with-covid-job-loss/
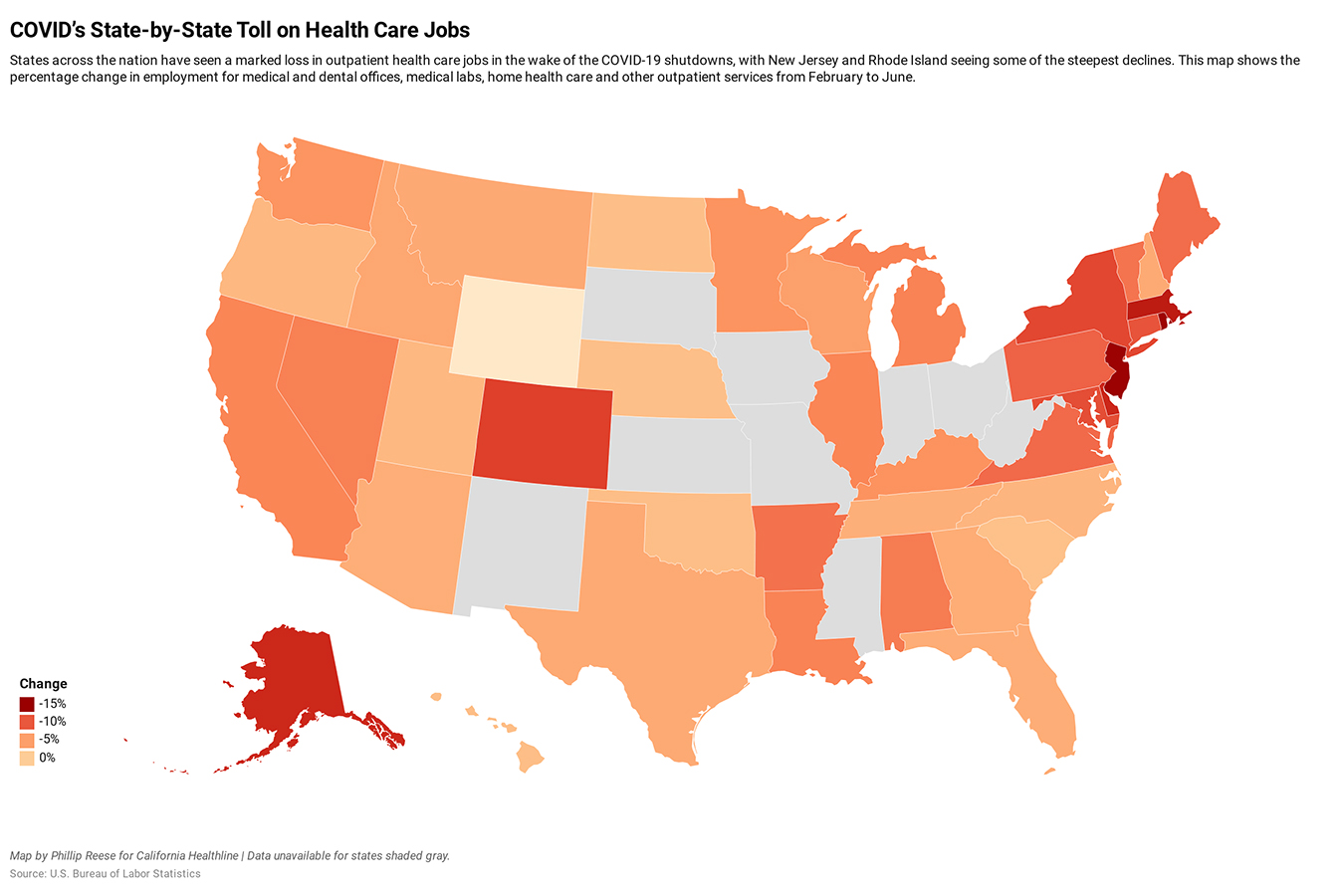
California’s outpatient health care practices largely shrugged off two recessions, adding more than 400,000 jobs during a two-decade climb from the start of 2000 to early 2020. It was an enviable growth rate of 85% and a trend largely mirrored on the national level.
Then came COVID-19.
Anecdotal stories abound about the crushing impact the pandemic has had on a range of outpatient medical services, from pediatric and family medical practices to dental offices, medical labs and home health care. In California, as in many other states, thousands of doctors, dentists and other health care providers temporarily closed offices this spring as state health officials directed them to suspend non-urgent visits. Many others sat open but largely idle because patients were too scared to visit the doctor given the risk of running into someone with COVID-19 in the waiting room.
As the economy has reopened, so have many medical offices. But the latest state and federal employment data underscores the lingering toll the pandemic has taken on the health care sector.
In California, and across the nation, the number of workers in doctors’ offices grew by more than 50% in the past 20 years, before seeing rapid declines amid COVID-19. This chart shows proportional growth in employment over time, with percentages relative to January 2000.
In California, employment in medical offices providing an array of outpatient care fell by 159,300 jobs, or 18%, from February to April, according to California’s Employment Development Department. The sector has recovered some, but job totals in June remained 7% below pre-crisis levels, the latest figures show. Data is not yet available for July, when COVID-19 cases in California again began to rise sharply and communities across much of the state reverted to partial shutdowns.
Nationwide, employment in outpatient care fell by about 1.3 million jobs, or 17%, from February to April, and in June also remained 7% below pre-crisis levels.
Doctors’ offices typically rely on patient volume for revenue. Without it, they can’t make payroll. Many small medical clinics weren’t flush with cash before the crisis, making COVID-19 an existential threat.
“Never in our history have we had more than a month’s cash on hand,” said Dr. Sumana Reddy, owner of the Acacia Family Medical Group in Monterey County. “Think of it that way.”
Reddy operates two clinics, one in Salinas and the other in the town of Prunedale. Many of her clients come from rural areas where poverty is common. When COVID-19 hit and stay-at-home orders took effect, the number of patients coming to the practice fell by about 50%, Reddy said. To keep her patients safe and her business afloat, Reddy largely shifted to telehealth so she could provide care online.
She also turned to federal aid. “I took the stimulus money,” she said. “I asked for advances from anywhere I could get that. So, now I’m tapped out. I’ve done every single thing that I can think of to do. And there’s nothing more to do.”
By late June, patient volume at Reddy’s practice stood at roughly 70% of the level seen before the crisis.
The coronavirus pandemic prompted steep declines in dental office employment, undoing 20 years of steady growth. This chart shows proportional growth in dental employment over time, with percentages relative to January 2000.
Many dental offices have been hit even harder. From February to April, the number of dental office employees in California fell by 85,000, or 60%, a rate of decline that outpaced even job losses in the state’s restaurant industry. Nationwide, dental employment fell by about 546,000 from February to April, a 56% decline.
“March, April, mid-May — we were pretty much closed except for emergency care,” said Dr. Natasha Lee, who owns Better Living Through Dentistry, a practice in San Francisco’s Inner Sunset neighborhood. “While dental offices were considered essential, most were closed due to guidance from health departments and the CDC to postpone routine and preventative medical and dental care and just to limit things to emergency.”
Lee has reopened her clinic but is doing less business. She and her staff need extra time to clean tools and change their personal protective equipment.
“With the social distancing, the limiting [of] patients in the office at a time and the slowdown we’ve had, we’re probably seeing about, I’d say, two-thirds of our normal capacity in our practice,” she said in late June.
As for employment, California hospitals have fared better than outpatient medical offices. Hospitals shed about 2% of jobs from February to June.
“They have more capacity in a large organization to withstand the same shock,” said John Romley, a professor and economist at the University of Southern California’s Leonard D. Schaeffer Center for Health Policy and Economics.
Romley said he is optimistic the health care sector overall will recover faster than some other sectors of the economy, since health care remains a necessity.
Still, red flags abound. The recent spike in COVID-19 cases and deaths in many parts of the nation raises the specter of future shutdowns and, with them, additional health care layoffs. In California, Gov. Gavin Newsom recently ordered a second shutdown for dine-in restaurants, movie theaters and bars statewide, as well as churches, gyms and barbershops in much of the state. For now, dental and doctors’ offices can continue operating.
A recent census survey found that 42% of California respondents had put off medical care because of the pandemic.
But it’s uncertain when patients will feel comfortable returning to the doctor for routine and preventive care. A series of Census Bureau surveys conducted between June 11 and July 7 found that 42% of Californians who responded had put off medical care in the previous four weeks because of the pandemic. About 33% said they needed medical care for something unrelated to COVID-19 but did not get it.
“I’ve been telling my staff and patients that we should prepare for things to stay not too different for six months to a year,” Reddy said, “which is pretty depressing for most people to think about.”

While many hospitals have devised ways to stretch material resources — converting surgery wards into specialized covid units and recycling masks and gowns — it is far more difficult to stretch the human workers needed to make the system function.
“At the end of the day, the capacity for critical care is a balance between the space, staff and stuff. And if you have a bottleneck in one, you can’t take additional patients,” said Mahshid Abir, a senior physician policy researcher at the RAND Corporation and director of the Acute Care Research Unit (ACRU) at the University of Michigan. “You have to have all three … You can’t have a ventilator, but not a respiratory therapist.”
“What this is going to do is it’s going to cost lives, not just for covid patients, but for everyone else in the hospital,” she warned.
The increasingly fraught situation reflects packed hospitals across large swaths of the country: More than 8,800 covid patients are hospitalized in Texas; Florida has more than 9,400; and at least 13 other states also have thousands of hospitalizations, according to data compiled by The Washington Post.
Facilities in several states, including Texas, South Carolina and Indiana, have in recent weeks reported shortages of such workers, according to federal planning documents viewed by The Post, pitting states and hospitals against one another to recruit staff.
On Thursday, Louisiana Gov. John Bel Edwards (D) said he asked the federal government to send in 700 health-care workers to assist besieged hospitals.
“Even if for some strange reason … you don’t care about covid-19, you should care about that hospital capacity when you have an automobile accident or when you have your heart attack or your stroke, or your mother or grandmother has that stroke,” Edwards said at a news conference.
In Florida, 39 hospitals have requested help from the state for respiratory therapists, nurses and nursing assistants. In South Carolina, the National Guard is sending 40 medical professionals to five hospitals in response to rising cases.
Many medical facilities anticipate their staffing problems will deteriorate, according to the planning documents: Texas is hardest hit, with South Carolina close behind. Needs range from pharmacists to physicians.
Hot spots stretch across the country, from Miami and Atlanta to Southern California and the Rio Grande Valley, and the demands for help are as diffuse as the suffering.
“What we have right now are essentially three New Yorks with these three major states,” White House coronavirus task force coordinator Deborah Birx said Friday during an appearance on NBC’s “Today” show.
But today’s diffuse transmission requires innovative thinking and a different response from months ago in New York, say experts. While some doctors have been able to share expertise online and nurses have teamed up to relieve pressures, the overall strains are growing.
“We missed the boat,” said Serena Bumpus, a leader of multiple Texas nursing organizations and regional director of nursing for the Austin Round Rock Region of Baylor Scott and White Health.
Bumpus blames a lack of coordination at national and state officials. “It feels like this free-for-all,” she said, “and each organization is just kind of left up to their own devices to try to figure this out.”
In a disaster, a hospital or local health system typically brings in help from neighboring communities. But that standard emergency protocol, which comes into play following a hurricane or tornado, “is predicated on the notion that you’ll have a concentrated area of impact,” said Christopher Nelson, a senior political scientist at the RAND Corporation and a professor at the Pardee RAND Graduate School.
That is how Texas has functioned in the past, said Jennifer Banda, vice president of advocacy and public policy at the Texas Hospital Association, recalling the influx of temporary help after Hurricane Harvey deluged Houston three years ago.
It is how the response took shape early in the outbreak, when health-care workers headed to hard-hit New York.
But the sustained and far-flung nature of the pandemic has made that approach unworkable. “The challenge right now,” Banda said, “is we are taxing the system all across the country.”
Theresa Q. Tran, an emergency medicine physician and assistant professor of emergency medicine at Houston’s Baylor College of Medicine, began to feel the crunch in June. Only a few weeks before, she had texted a friend to say how disheartening it was to see crowds of people reveling outdoors without masks on Memorial Day weekend.
Her fears were borne out when she found herself making call after call after call from her ER, unable to admit a critically ill patient because her hospital had run out of ICU space, but unable to find a hospital able to take them.
Under normal circumstances, the transfer of such patients — “where you’re afraid to look away, or to blink, because they may just crash on you,” as Tran describes them — happens quickly to ensure the close monitoring the ICU affords.
Those critical patients begin to stall in the ER, stretching the abilities of the nurses and doctors attending to them. “A lot of people, they come in, and they need attention immediately,” Tran said, noting that emergency physicians are constantly racing against time. “Time is brain, or time is heart.”
By mid-July, an influx of “surge” staff brought relief, Tran said. But that was short-lived as the crisis jumped from one locality to the next, with the emergency procedures to bring in more staff never quite keeping up with the rising infections.
An ER physician in the Rio Grande Valley said all three of the major trauma hospitals in the area have long since run out of the ability to absorb new ICU patients.
“We’ve been full for weeks,” said the physician, who spoke on the condition of anonymity because he feared retaliation for speaking out about the conditions.
“The truth is, the majority of our work now in the emergency department is ICU work,” he said. “Some of our patients down here, we’re now holding them for days.” And each one of those critically ill patients needs a nurse to stay with them.
When ICU space has opened up — maybe two, three, four beds — it never feels like relief, he said, because in the time it takes to move those patients out, 20 new ones arrive.
Even with help his hospital has received — masks and gowns were procured, and the staff more than doubled in the past few weeks with relief nurses and other health-care workers from outside — it still is not enough.
The local nurses are exhausted. Some quit. Even the relief nurses who helped out in New York in the spring seem horrified by the scale of the disaster in South Texas, he said.
“If no one comes and helps us out and gives us the ammo we need to fight this thing, we are not going to win,” the doctor said.
One of the root causes of the problem in the United States is that emergency departments and ICUs are often operating at or near capacity, Abir and Nelson said, putting them dangerously close to shortages before a crisis even hits.
Texas, along with 32 other states, has joined a licensure compact, allowing nurses to practice across state borders, but it is becoming increasingly difficult to recruit from other parts of the country.
Texas medical facilities can apply to the Department of State Health Services for staffers to fill a critical shortage, typically for a two-week period. But two weeks, which would allow time to respond to most disasters, hardly registers in a pandemic, so facilities have to ask for extensions or make new applications.
South Carolina last week issued an order that allows nursing graduates who have not yet completed their licensing exams to begin working under supervision. Prisma Health, the state’s biggest hospital system, said this week that the number of patients admitted to its hospitals has more than tripled in the past three weeks and is approaching 300 new patients a day.
“As the capacity increases, so does the need for additional staff,” Scott Sasser, the incident commander for Prisma Health’s covid-19 response said in a statement. Prisma has so far shifted nurses from one area to another, brought back furloughed nurses, hired more physicians and brought in temporary nurse hires, among other measures, Sasser said.
Bumpus has fielded calls from nurses all over the country — some as far afield as the United Kingdom — wanting to know how they can help. But Bumpus says she does not have an easy answer.
“I’ve had to kind of just do my own digging and use my connections,” she said. At first, she said, interested nurses were asked to register through the Texas Disaster Volunteer Registry; but then the system never seemed to be put to use.
Later she learned — “by happenstance … literally by social media” — that the state had contracted with private agencies to find nurses. So now she directs callers to those agencies.
Even rural parts of Texas that were spared initially are being ravaged by the virus, according to John Henderson, CEO of the Texas Organization of Rural and Community Hospitals.
“Unless things start getting better in short order, we don’t have enough staff,” he acknowledged. As for filling critical staffing gaps by moving people around, “even the state admits that they can’t continue to do that,” Henderson said.
The situation has become so dire in some rural parts of the state that Judge Eloy Vera implored people to stay home on the Starr County Facebook page, warning, “Unfortunately, Starr County Memorial Hospital has limited resources and our doctors are going to have to decide who receives treatment, and who is sent home to die.”
Steven Gularte, CEO of Chambers Health in Anahuac, Tex., 45 miles from Houston, said he had to bring in 10 nurses to help staff his 14-bed hospital after Houston facilities started appealing for help to care for patients who no longer needed intensive care but were not ready to go home.
“Normally, we are referring to them,” Gularte said. “Now, they are referring to us.”
Donald M. Yealy, chair of emergency medicine at the University of Pittsburgh Medical Center, said rather than sending staff to other states, his hospital has helped others virtually, particularly to support pulmonary and intensive care physicians.
“Covid has been catalytic in how we think about health care,” Yealy said, providing lessons that will outlast the pandemic.
But telehealth can do little to relieve the fatigue and fear that goes with front-line work in a prolonged pandemic. Donning and doffing masks, gowns and gloves is time consuming. Nurses worry about taking the virus home to their families.
“It is high energy work with a constant grind that is hard on people,” said Michael Sweat, director of the Center for Global Health at the Medical University of South Carolina.
Coronavirus has turned the regular staffing challenge at Harris Health in Houston into a daily life-or-death juggle for Pamela Russell, associate administrator of nursing operations, who helps provide supplemental workers for the system’s two public hospitals and 46 outpatient clinics.
Now, 162 staff members — including more than 50 nurses — are quarantined, either because they tested positive or are awaiting results. Many others need flexible schedules to accommodate child care, she said. Some cannot work in coronavirus units because of their own medical conditions. A few contract nurses left abruptly after learning their units would soon be taking covid-positive patients.
Russell has turned to the state and the international nonprofit Project Hope for resources, even as she acts as a morale booster, encouraging restaurants to send meals and supporting the hospital CEO in his cheerleading rounds.
“It’s hard to say how long we can do this. I just don’t know” said Russell, who praised the commitment of the nurses. “Like I said, it’s a calling. But I don’t see it being sustainable.”
https://mailchi.mp/9075526b5806/the-weekly-gist-july-24-2020?e=d1e747d2d8

We got an update from the chief medical information officer of one of our member systems about their ongoing progress in expanding telemedicine. Their rate of virtual visits peaked in late April, accounting for over half of all physician encounters. But like most systems, they’ve seen telemedicine visits drop to less than 20 percent of all appointments as physician offices have reopened.
In thinking about how the system will move telemedicine forward, she said, “We’re trying to be intentional and really design a top-notch consumer experience, with quality as the foundation.” They are going specialty-by-specialty, condition-by-condition, to redesign care pathways to optimally blend virtual and in-person care. It’s daunting, but she believes COVID-19 provided a model for how to do this quickly and effectively.
In just a few weeks, many systems stood up COVID management programs in the following way: algorithm-driven, online symptom triage triggers a virtual visit with a doctor. Testing is conducted at new, dedicated locations, to keep doctors’ offices as COVID-free as possible. Patients with concerning symptoms are monitored at home with pulse oximetry and regular check-ins; the same resources are used to ensure discharged patients are recovering well.
It’s the perfect example of how to design a safe, consumer-centered care pathway, using the whole of a health system’s resources. Now the challenge facing doctors and hospitals is: can this process be scaled across the hundreds of conditions that could benefit from a blend of virtual and traditional care?
https://mailchi.mp/9075526b5806/the-weekly-gist-july-24-2020?e=d1e747d2d8

Last week we wrote about an observation from some physician leaders that, paradoxically, physician burnout seemed to have waned a bit during the COVID crisis. They felt that, as clinicians rallied to provide care for patients during the pandemic, many found new purpose in the work, despite great challenges. Bureaucratic hurdles yielded to the need to make critical decisions quickly, as did regulatory barriers to telemedicine.
The piece sparked a number of doctors, most from regions now experiencing surges, to share their alternative viewpoints with us.
One employed physician wrote that, across specialties, he and his colleagues are angry. They don’t feel protected, either financially, or even for their own physical safety.
A nurse practitioner working long shifts in an emergency department overloaded with COVID patients wrote, “In April, I would have never believed that we would be scrounging for PPE at the end of July. How could this happen?” And a nephrologist redeployed to a COVID ICU shared: “With the surge in New York, it felt like the entire country was behind their doctors and nurses. I drive home past restaurants and stores filled with people refusing to wear masks. It’s so demoralizing.”
Several expressed that their employers, both health systems and payers, are “counting on our goodwill that we’ll just keep showing up.” But once the crisis passes, there may be “drastic and irrational physician revolts. Someone should be watching for it.”
These comments reveal a marked difference in physician sentiment in different parts of the country, based both on the severity of the pandemic, and the nature of the local response. Regardless, we’d agree that the clinical workforce, both doctors and nurses, is working through a period of unprecedented stress, and for some, emotional trauma. Ensuring their stability and safety must be a top priority for every health system and medical group.

COVID-19 has led to a boom in telehealth, with some health care facilities seeing an increase in its use by as much as 8,000%.
This shift happened quickly and unexpectedly and has left many people asking whether telehealth is really as good as in-person care.
Over the last decade, I’ve studied telehealth as a Ph.D. researcher while using it as a registered nurse and advanced practice nurse. Telehealth is the use of phone, video, internet and technology to perform health care, and when done right, it can be just as effective as in-person health care. But as many patients and health care professionals switch to telehealth for the first time, there will inevitably be a learning curve as people adapt to this new system.
So how does a patient or a provider make sure they are using telehealth in the right way? That is a question of the technology available, the patient’s medical situation and the risks of going – or not going – to a health care office.

There are three main types of telehealth: synchronous, asynchronous and remote monitoring. Knowing when to use each one – and having the right technology on hand – is critical to using telehealth wisely.
Synchronous telehealth is a live, two-way interaction, usually over video or phone. Health care providers generally prefer video conferencing over phone calls because aside from tasks that require physical touch, nearly anything that can be done in person can be done over video. But some things, like the taking of blood samples, for example, simply cannot be done over video.
Many of the limitations of video conferencing can be overcome with the second telehealth approach, remote patient monitoring. Patients can use devices at home to get objective data that is automatically uploaded to health care providers. Devices exist to measure blood pressure, temperature, heart rhythms and many other aspects of health. These devices are great for getting reliable data that can show trends over time. Researchers have shown that remote monitoring approaches are as effective as – and in some cases better than – in-person care for many chronic conditions.
Some remaining gaps can be filled with the third type, asynchronous telehealth. Patients and providers can use the internet to answer questions, describe symptoms, refill prescription refills, make appointments and for other general communication.
Unfortunately, not every provider or patient has the technology or the experience to use live video conferencing or remote monitoring equipment. But even having all the available telehealth technology does not mean that telehealth can solve every problem.

Generally, telehealth is right for patients who have ongoing conditions or who need an initial evaluation of a sudden illness.
Because telehealth makes it easier to have have frequent check-ins compared to in-person care, managing ongoing care for chronic illnesses like diabetes, heart disease and lung disease can be as safe as or better than in-person care.
Research has shown that it can also be used effectively to diagnose and even treat new and short-term health issues as well. The tricky part is knowing which situations can be dealt with remotely.
Imagine you took a fall and want to get medical advice to make sure you didn’t break your arm. If you were to go to a hospital or clinic, almost always, the first health care professional you’d see is a primary care generalist, like me. That person will, if possible, diagnose the problem and give you basic medical advice: “You’ve got a large bruise, but nothing appears to be broken. Just rest, put some ice on it and take a pain reliever.” If I look at your arm and think you need more involved care, I would recommend the next steps you should take: “Your arm looks like it might be fractured. Let’s order you an X-ray.”
This first interaction can easily be done from home using telehealth. If a patient needs further care, they would simply leave home to get it after meeting with me via video. If they don’t need further care, then telehealth just saved a lot of time and hassle for the patient.
Research has shown that using telehealth for things like minor injuries, stomach pains and nausea provides the same level of care as in-person medicine and reduces unnecessary ambulance rides and hospital visits.
Some research has shown that telehealth is not as effective as in-person care at diagnosing the causes of sore throats and respiratory infections. Especially now during the coronavirus pandemic, in-person care might be necessary if you are having respiratory issues.
And finally, for obviously life-threatening situations like severe bleeding, chest pain or shortness of breath, patients should still go to hospitals and emergency rooms.

With the right technology and in the right situations, telehealth is an incredibly effective tool. But the question of when to use telehealth must also take into account the risk and burden of getting care.
COVID-19 increases the risks of in-person care, so while you should obviously still go to a hospital if you think you may be having a heart attack, right now, it might be better to have a telehealth consultation about acne – even if you might prefer an in-person appointment.
Burden is another thing to consider. Time off work, travel, wait times and the many other inconveniences that go along with an in-person visit aren’t necessary simply to get refills for ongoing medication. But, if a provider needs to draw a patient’s blood to monitor the safety or effectiveness of a prescription medicine, the burden of an in-person visit to the lab is likely worth the increased risk.
Of course, not all health care can be done by telehealth, but a lot can, and research shows that in many cases, it’s just as good as in-person care. As the pandemic continues and other problems need addressing, think about the right telehealth fit for you, and talk to your health care team about the services offered, your risks and your preferences. You might find that that there are far fewer waiting rooms in your future.

