The coronavirus has decimated the U.S. economy and benched nearly 40 million American workers. In the past several days, the U.S. has logged its highest number of new Covid-19 cases since the pandemic began. These combined with other factors, which we will discuss, is jeopardizing the future employment of millions of workers and the viability of thousands of businesses. Here’s how unemployment has increased for every state, industry, age group, and race, and why.
Unemployment by State
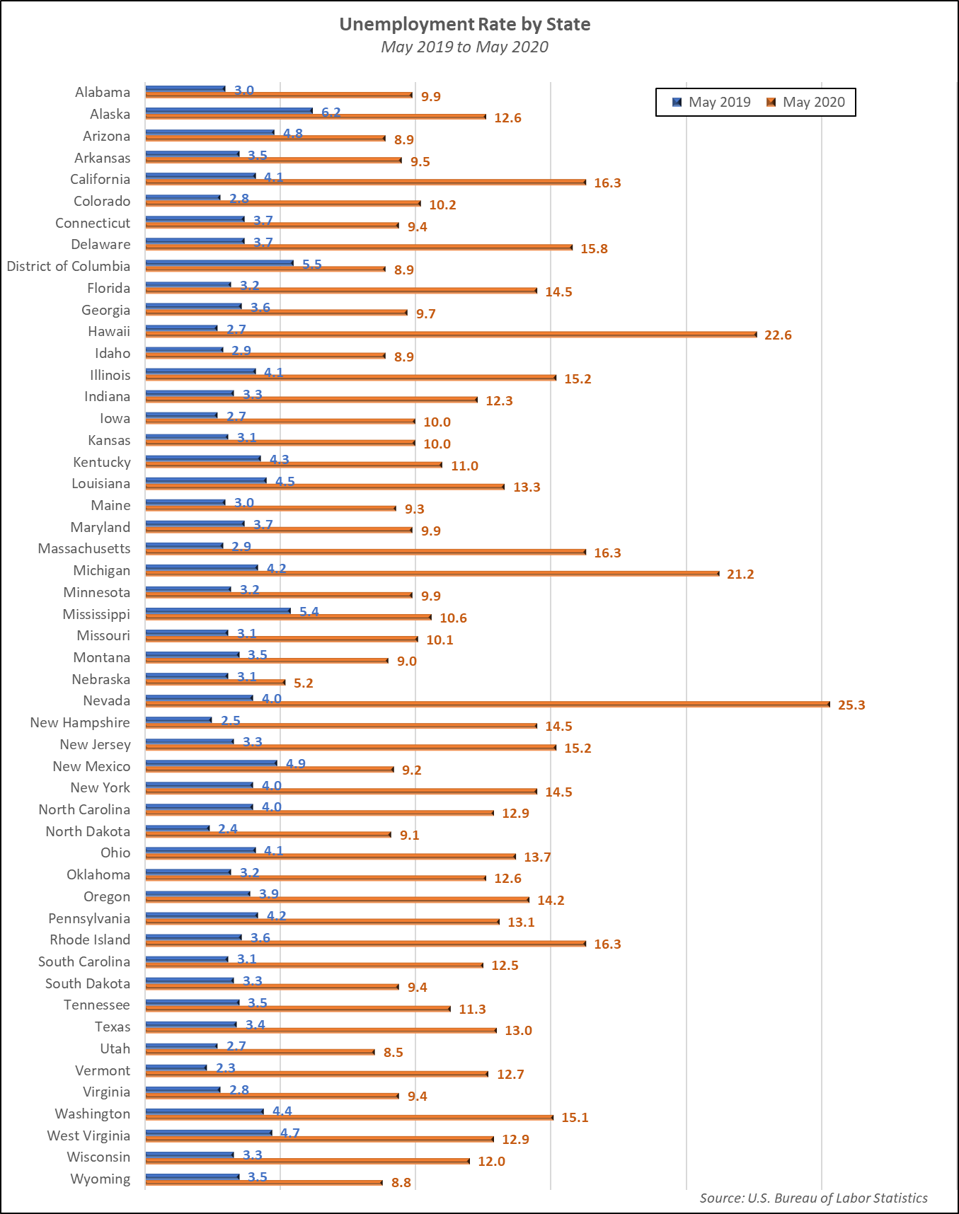
The coronavirus and subsequent stay at home orders hit the labor force especially hard. As states attempted to reopen, a resurgence in the virus is causing many businesses to close again, some by choice, others by government mandate.
Nevada has been hit the hardest as the unemployment rate in the Silver State rose from 4.0% in May 2019 to a whopping 25.3% in May 2020. Nevada’s economy is heavily reliant on leisure and hospitality, which had the brunt of the job losses. Hawaii, the second hardest hit state saw unemployment rise from 2.7% in May 2019 to 22.6% in May 2020. Which is the only other state with unemployment above 20% in May 2020? Michigan, where unemployment rose from 4.2% to 21.2% year over year. What state has fared best? Nebraska, which also has one of the most diverse economies of all states. Deriving nearly 50% of its total GDP from five different industries, unemployment in the Cornhusker State rose from 3.1% to a modest 5.2% from May 2019 to May 2020. Unemployment numbers for all states are shown in the following chart.
Unemployment by Industry
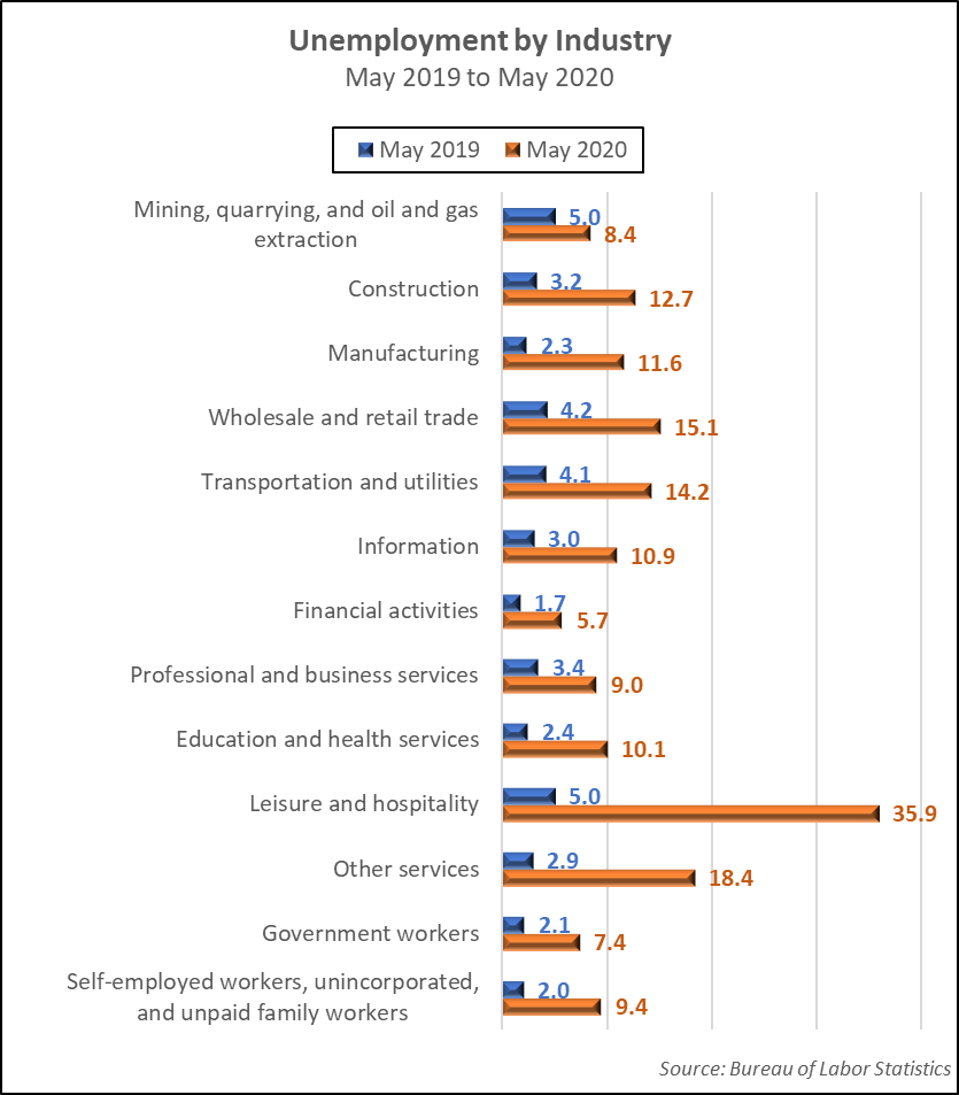
As mentioned in the previous section, the states that have fared best either have a more diverse economy or do not rely heavily on industries that have been hardest hit by the coronavirus. The most negatively affected is the leisure and hospitality industry where unemployment rose 618% from a low of 5.0% in May 2019 to a staggering 35.9% in May 2020. At a distant second, but still reeling, is the wholesale and retail trade industry, which saw unemployment rise from 4.2% to 15.1% during the same period. The rest of the industries are listed in the following chart.
Unemployment by Age Group
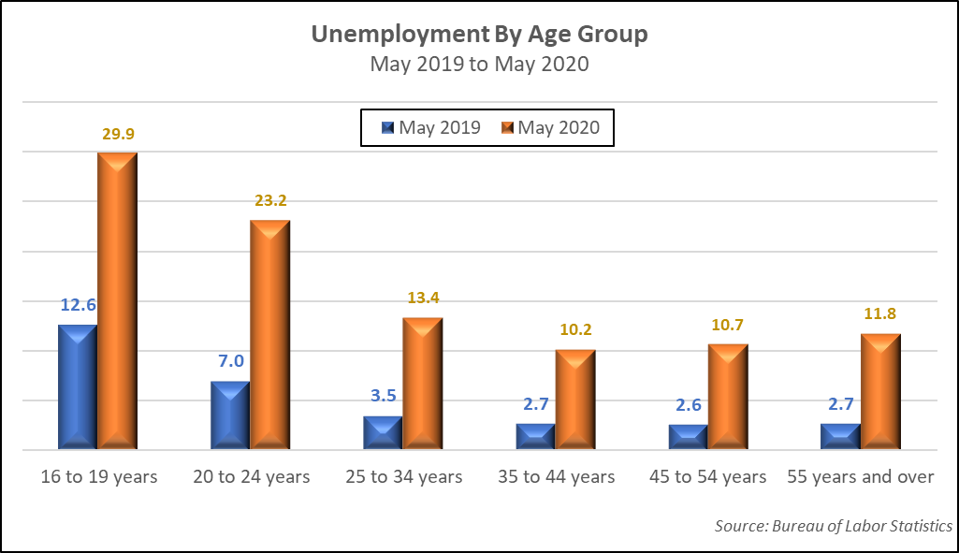
Businesses need two things to exist: workers and customers. Without customers, there is no need for workers or the business for that matter. Some businesses require highly skilled workers while others operate well using unskilled labor. It is this unskilled labor group that has been hardest hit.
The greatest rise in unemployment is among workers under age 25. This is likely due to three factors. Younger workers typically have fewer marketable skills, less work experience, and less seniority. Many of these workers are in industries that have felt the greatest pain. Unemployment rates by age group are contained in the following chart.
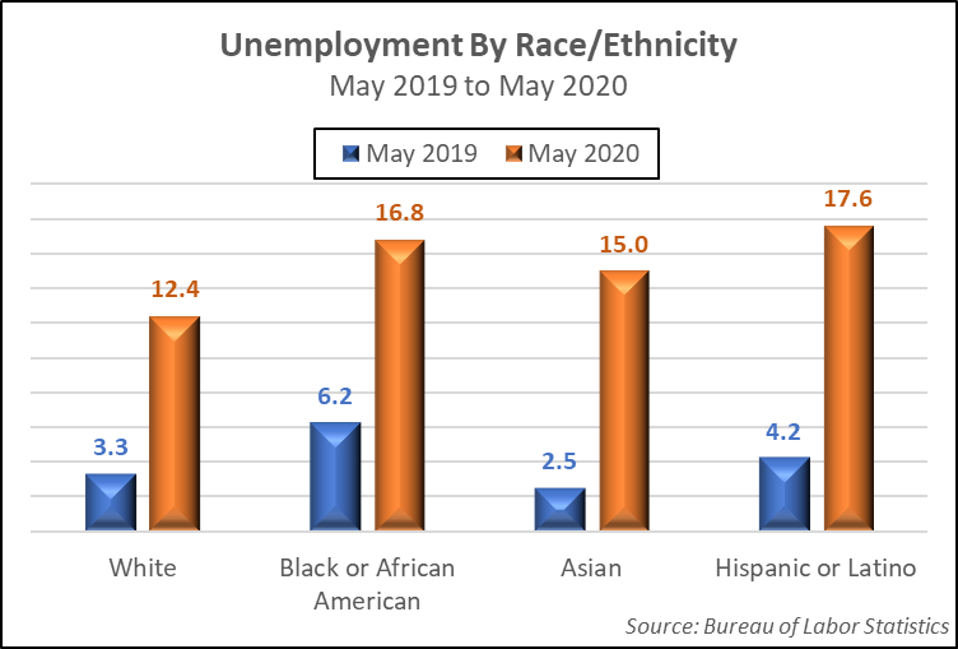
Unemployment by Race/Ethnicity
Question: Prior to Covid-19, was unemployment among blacks / African Americans at a record low as President Trump has claimed? Using the available data, which extends back to January 1972, the answer is yes. This new record low was achieved in October and November of 2019 when unemployment among black or African American workers fell to 5.1%. The previous record low was 5.2% in December 1973. The current rate is 16.8%, which is less than the highest rate of 20.7% logged in December 1982. The most recent high in unemployment for this group was 19.3% in March 2010. It has been steadily declining since then. Numbers for White, Asian, and Hispanic or Latino and black or African American workers are listed in the following chart.
Businesses need workers, workers need businesses, and both depend on customers. Since the pandemic began, consumer demand has fallen sharply. With the probability that a vaccine will not be available until early 2021 at the soonest, plus a disregard for recommended safety protocols by many individuals, namely wearing masks and social distancing, it is highly unlikely that the economy will return to normal for several years.
Will the president continue to hold rallies? Will he set an example by wearing a mask? Will the protests and violence continue? Will other large gatherings continue? Unless Americans make a collective and conscious choice to mask up and social distance, we will be forced to live in a depressed economy for longer than necessary. The choice is up to us.